HNY Policy and Pathway Repository - York
Non-visible haematuria
Definition/Description
NVH: |
Presence of blood on dipstick testing- score of +1 or greater counted as positive. |
Persistent NVH: |
Two out of three or more positive urine dips separated in time by 2 weeks and spurious causes excluded, ignore trace readings. |
Symptomatic NVH: |
As above with voiding lower urinary tract symptoms such as hesitancy, frequency, urgency, dysuria and loin or supra-pubic pain in the absence of a transient cause such as UTI. |
Spurious Causes: |
Menstruation, Sexual intercourse, Foods – beetroot, blackberries, rhubarb, Rhabdomyolysis, Drugs – doxorubicin, chloroquine, rifampicin, Lead/mercury poisoning, DOACs, Warfarin. |
Transient causes: |
UTI: (recurrent UTI infections over age 60, are an indication for further investigation, regardless of haematuria, defined as >3 infections) Exercise (march) haematuria: Repeat dipstick at least 3 days after activity to make sure resolved. |
Red Flag Symptoms
- Visible (frank) haematuria (in adult) without UTI.
- Solid swelling in body of testis
- Palpable renal mass
- Elevated age specific PSA in men with ten year life expectancy
- High PSA (>20ng/ml) in man with clinically malignant prostate or bone pain
- Any suspected penile cancer
Guidelines on Management
Management
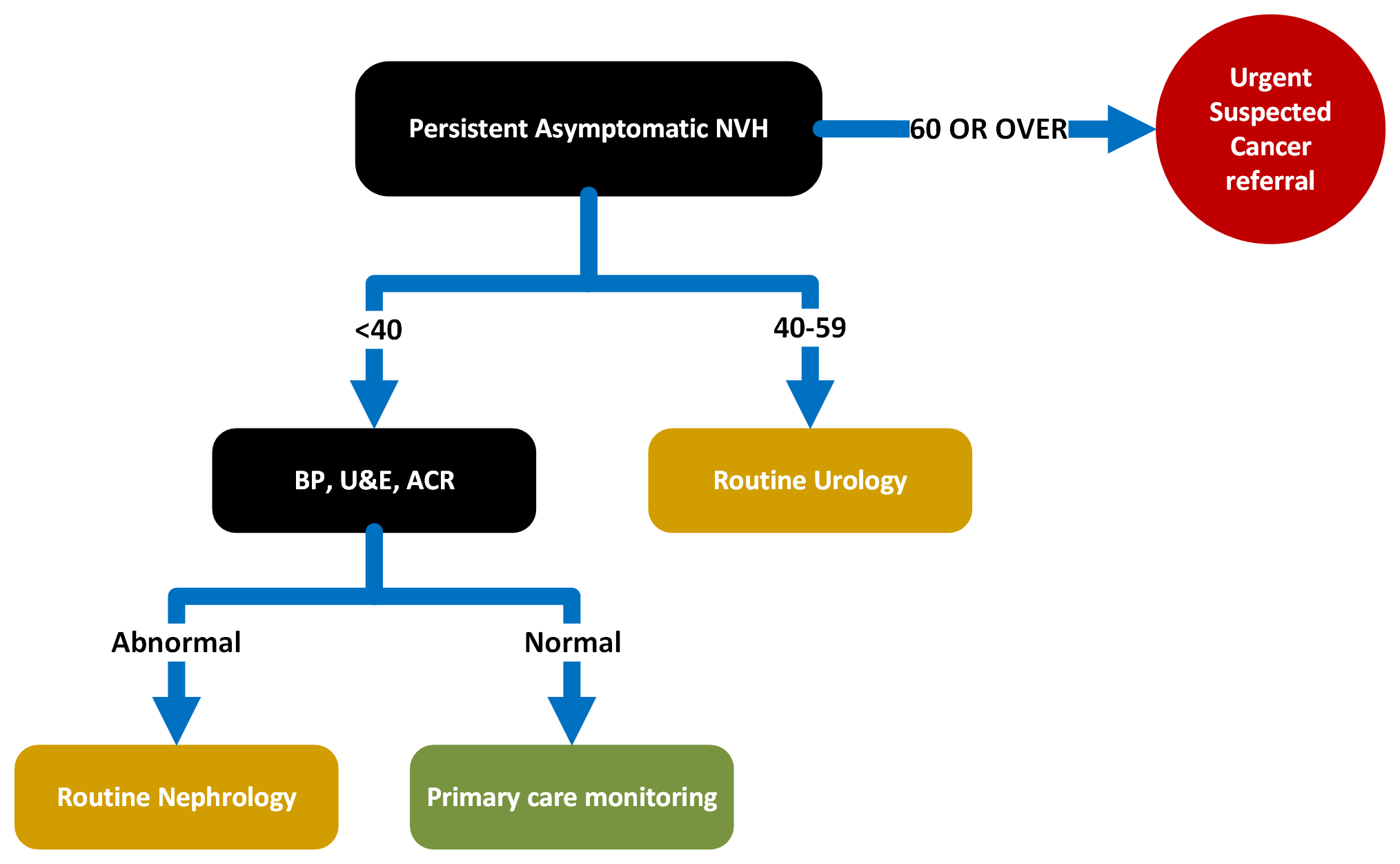
Exclude transient and spurious causes of NVH
See flowchart below.
Primary Care Monitoring (Annual Assessments)
Annual Review:
- Annual eGFR>60, ACR <30 and normal BP
Re-refer/refer urology if visible haematuria or symptomatic NVH develops.
Refer nephrology if:
- ACR increases >30 or PCR>50
- eGFR decreases to 5ml/min over 1 year or >10ml/min over 5 years)
Patients who have had negative urological investigations who persist with NVH should be discussed with nephrologist via A+G.
When to re-refer to Urology:
- Patients undergoing negative investigations for asymptomatic non-visible haematuria only require repeat Urological investigation if subsequently develop symptomatic NVH or visible haematuria
- Patients undergoing negative investigations for symptomatic non-visible haematuria only require repeat Urological investigation if subsequently develop visible haematuria
- Recurrent visible haematuria beyond 6 month mark since previous investigations, suggest re-referral for repeat investigations (haematuria clinic). GP may wish to liaise with initial Urologist.
- Consider requesting a CT urogram (or speaking to Urologist) if the visible haematuria recurs within 6 months of the initial investigations
Referral Criteria/Information
Information to include in referral letter
- Evidence that transient or spurious causes of NVH have been excluded
- Relevant past medical / surgical history
- Current regular medication
- BMI / Smoking status
Investigations prior to referral
- BP
- Creatinine, eGFR
- Urine ACR (albumin creatinine ratio)
- FBC, Clotting screen
Additional Resources & Reference
Associated Policies
Specialties
Places covered by
- Vale of York
Hospital Trusts
York and Scarborough Teaching Hospitals