HNY Policy and Pathway Repository - York
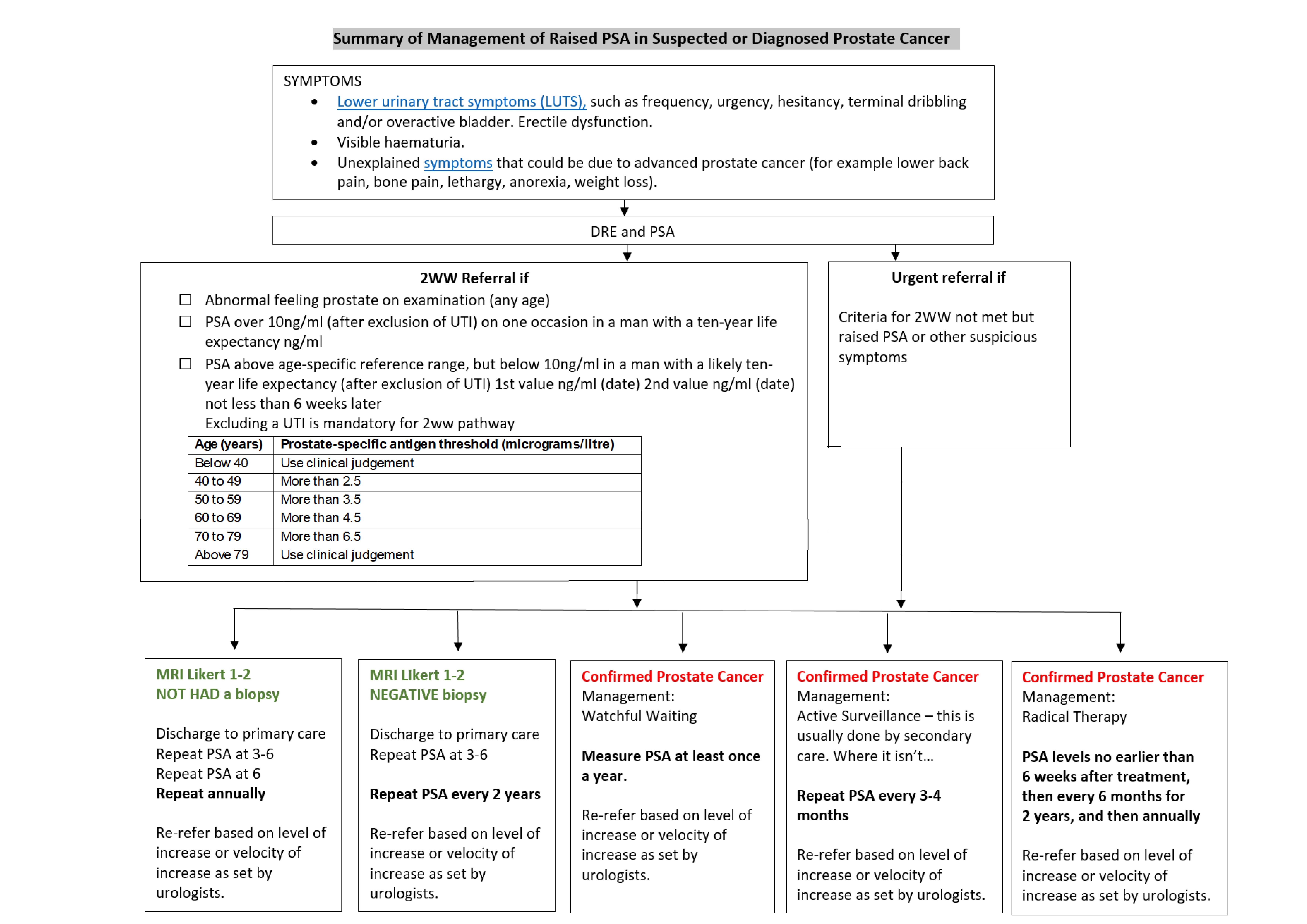
Management of raised PSA in suspected or diagnosed prostate cancer (following secondary care assessment)
Definition/Description
The Vale of York CCG has a Local Enhanced Service for primary care monitoring of patients with prostate cancer who need repeat PSAs.
Specific individual patient recommendations will be communicated to GPs via hospital letters. NICE NG131 (2019) includes recommendations on follow-up in primary care for people diagnosed with prostate cancer.
Red Flag Symptoms
None provided
Guidelines on Management
Radiologists give MRI images a score from 1 to 5. This is called the PI-RADS (Prostate Imaging – Reporting and Data System) score or a Likert score.
- PIRADS or Likert score 1-2 It’s very unlikely that you have prostate cancer that needs to be treated.
- PIRADS or Likert score 3 It isn’t possible to tell from the scan whether you have prostate cancer that needs to be treated – you may hear this called a borderline result.
- PIRADS or Likert score 4 It’s likely that you have prostate cancer that needs to be treated.
- PIRADS or Likert score 5 It’s very likely that you have prostate cancer that needs to be treated.
1. For people who have a raised PSA and MRI Likert score of 1 or 2, and who have not had a prostate biopsy, repeat PSA test at 3 to 6 months and:
- discharge the person to primary care if the level of suspicion is low;
- advise PSA follow-up at 6 months and then every year, and
- set a PSA level for primary care at which to re-refer based on PSA level or rate of change (velocity).
2. For people who have a raised PSA, an MRI Likert score of 1 or 2 (or a contraindication to MRI), and negative biopsy, repeat PSA at 3 to 6 months and:
- discharge the person to primary care if the level of suspicion is low;
- advise PSA follow-up every 2 years, and
- set a PSA level for primary care at which to re-refer, based on PSA level or rate of change (velocity).
3. Watchful waiting
This is part of a strategy for 'controlling' rather than 'curing' prostate cancer and is aimed at people with localised prostate cancer who do not ever wish to have curative treatment, or it is not suitable for them. Instead, it involves the deferred use of hormone therapy. Watchful waiting avoids the use of surgery or radiation, but implies that curative treatment will not be attempted.
Follow up people with prostate cancer who have chosen a watchful waiting regimen with no curative intent in primary care. Measure their PSA at least once a year, or as advised.
4. Active surveillance
This is part of a 'curative' strategy and is aimed at people with localised prostate cancer for whom radical treatments are suitable, keeping them within a 'window of curability' whereby only those whose tumours are showing signs of progressing, or those with a preference for intervention are considered for radical treatment. Active surveillance may thus avoid or delay the need for radiotherapy or surgery.
Year 1 of active surveillance: measure PSA every 3-4 months, or as advised.
5. Radical Therapy
The aim of radical therapy is to offer curative treatment, using either prostatectomy to remove the entire prostate gland or radiotherapy to eradicate the disease. Surgery can be performed by open, laparoscopic, or robot-assisted surgery, radiotherapy by external beam or brachytherapy. It’s an option for Localized prostate cancer, surgery is occasionally offered for biochemical relapse after radical radiotherapy.
Specialist healthcare professionals should advise thresholds for re-referral and provide these when discharging people, rather than expecting the calculations to be made in primary care.
The table on the next page summarises the management.
Referral Criteria/Information
See image A below.
Additional Resources & Reference
PSA testing - a quick one page summary
Prostate Cancer- PSA monitoring (enhanced service overview)
Patient information leaflets/PDAs
- The NICE Guideline NG 131 has a lot of helpful information on the investigation and management of suspected and confirmed Prostate Cancer and prognosis depending on diagnosed severity that many patients will find helpful.
- NHS A-Z
- Cancer Research UK
- Prostate Cancer UK
- Macmillan Cancer Support
NICE Quality Standards for Prostate Cancer
Statement 1: People with prostate cancer have a discussion about treatment options and adverse effects with a named nurse specialist.
Statement 2: People with low-risk localised prostate cancer for whom radical treatment is suitable are offered a choice between active surveillance, radical prostatectomy or radical radiotherapy.
Statement 3: People with intermediate- or high-risk localised prostate cancer who are offered non-surgical radical treatment are offered radical radiotherapy and androgen deprivation therapy in combination.
Statement 4: People with adverse effects of prostate cancer treatment are referred to specialist services.
Statement 5: People with hormone-relapsed metastatic prostate cancer have their treatment options discussed by the urological cancer multidisciplinary team.
References
NICE NG131 Prostate cancer: diagnosis and management May 2019
Associated Policies
Specialties
Places covered by
- Vale of York
Hospital Trusts
York and Scarborough Teaching Hospitals