HNY Policy and Pathway Repository - North Yorkshire
Suspected haematological cancer
Definition/Description
Suspected haematological cancer including myeloma pathway.
Red Flag Symptoms
Urgently telephone Haematology consultant at HDFT and make 2 week referral if
- Blood Count or film suggestive of acute leukaemia or chronic myeloid leukaemia
Guidelines on Management
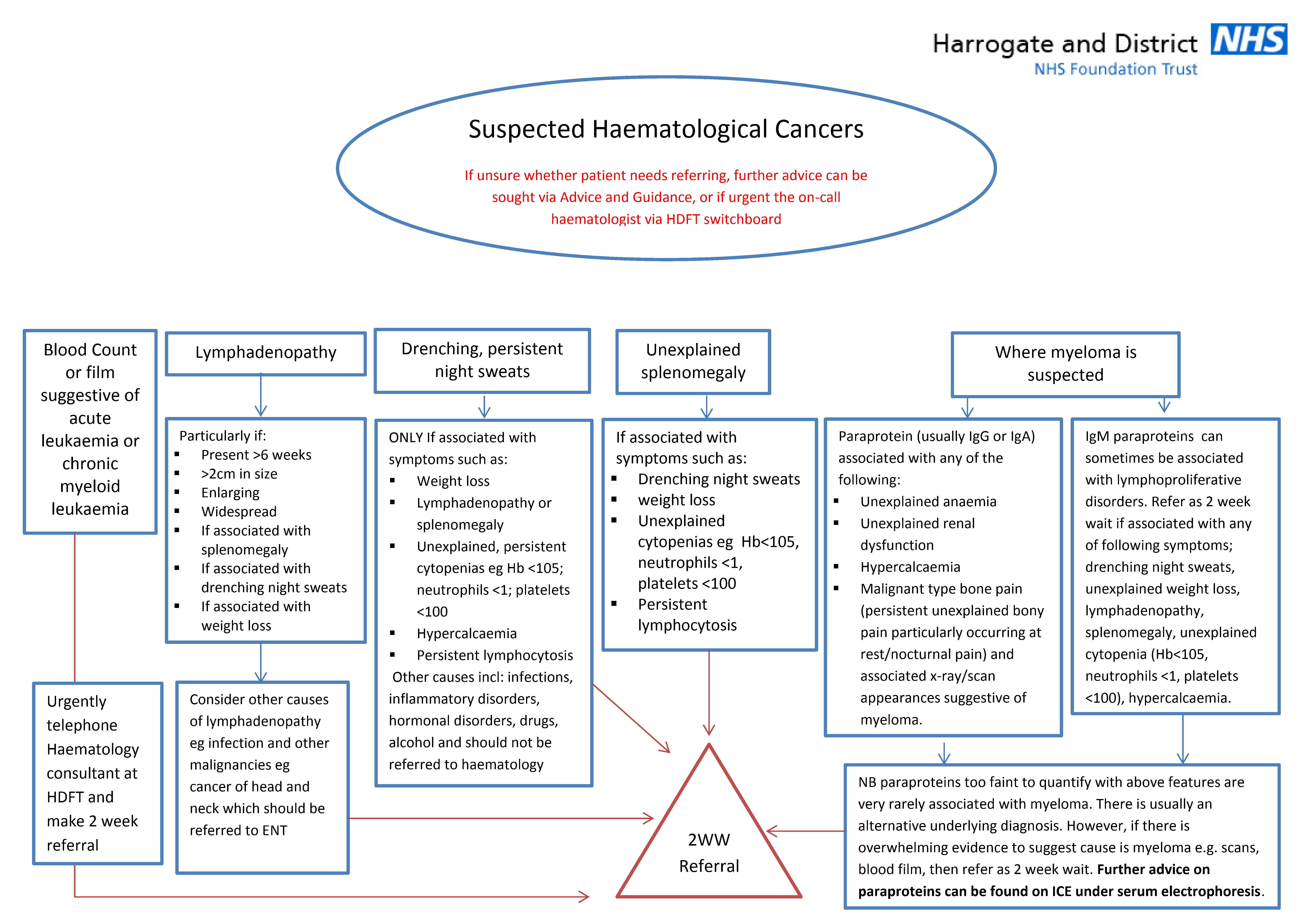
If unsure whether patient needs referring, further advice can be sought via Advice and Guidance, or if urgent the on-call haematologist via HDFT switchboard
Referral Criteria/Information
Refer as a USC haematology referral if has:
Lymphadenopathy
Particularly if:
- Present >6 weeks
- >2cm in size
- Enlarging
- Widespread
- If associated with splenomegaly
- If associated with drenching night sweats
- If associated with weight loss
Consider other causes of lymphadenopathy eg infection and other malignancies eg cancer of head and neck which should be referred to ENT
Drenching, persistent night sweats
ONLY If associated with symptoms such as:
- Weight loss
- Lymphadenopathy or splenomegaly
- Unexplained, persistent cytopenias eg Hb <105; neutrophils <1; platelets <100
- Hypercalcaemia
- Persistent lymphocytosis
Other causes incl: infections, inflammatory disorders, hormonal disorders, drugs, alcohol and should not be referred to haematology
Unexplained splenomegaly
If associated with symptoms such as:
- Drenching night sweats
- Weight loss
- Unexplained cytopenias eg Hb<105, neutrophils <1, platelets <100
- Persistent lymphocytosis
Myeloma
Where myeloma is suspected:
- Paraprotein (usually IgG or IgA) associated with any of the following:
- Unexplained anaemia
- Unexplained renal dysfunction
- Hypercalcaemia
- Malignant type bone pain (persistent unexplained bony pain particularly occurring at rest/nocturnal pain) and associated x-ray/scan appearances suggestive of myeloma.
- IgM paraproteins can sometimes be associated with lymphoproliferative disorders. Refer as 2 week wait if associated with any of following symptoms; drenching night sweats, unexplained weight loss, lymphadenopathy, splenomegaly, unexplained cytopenia (Hb<105, neutrophils <1, platelets <100), hypercalcaemia.
NB: paraproteins too faint to quantify with above features are very rarely associated with myeloma. There is usually an alternative underlying diagnosis. However, if there is overwhelming evidence to suggest cause is myeloma e.g. scans, blood film, then refer as 2 week wait. Further advice on paraproteins can be found on ICE under serum electrophoresis.
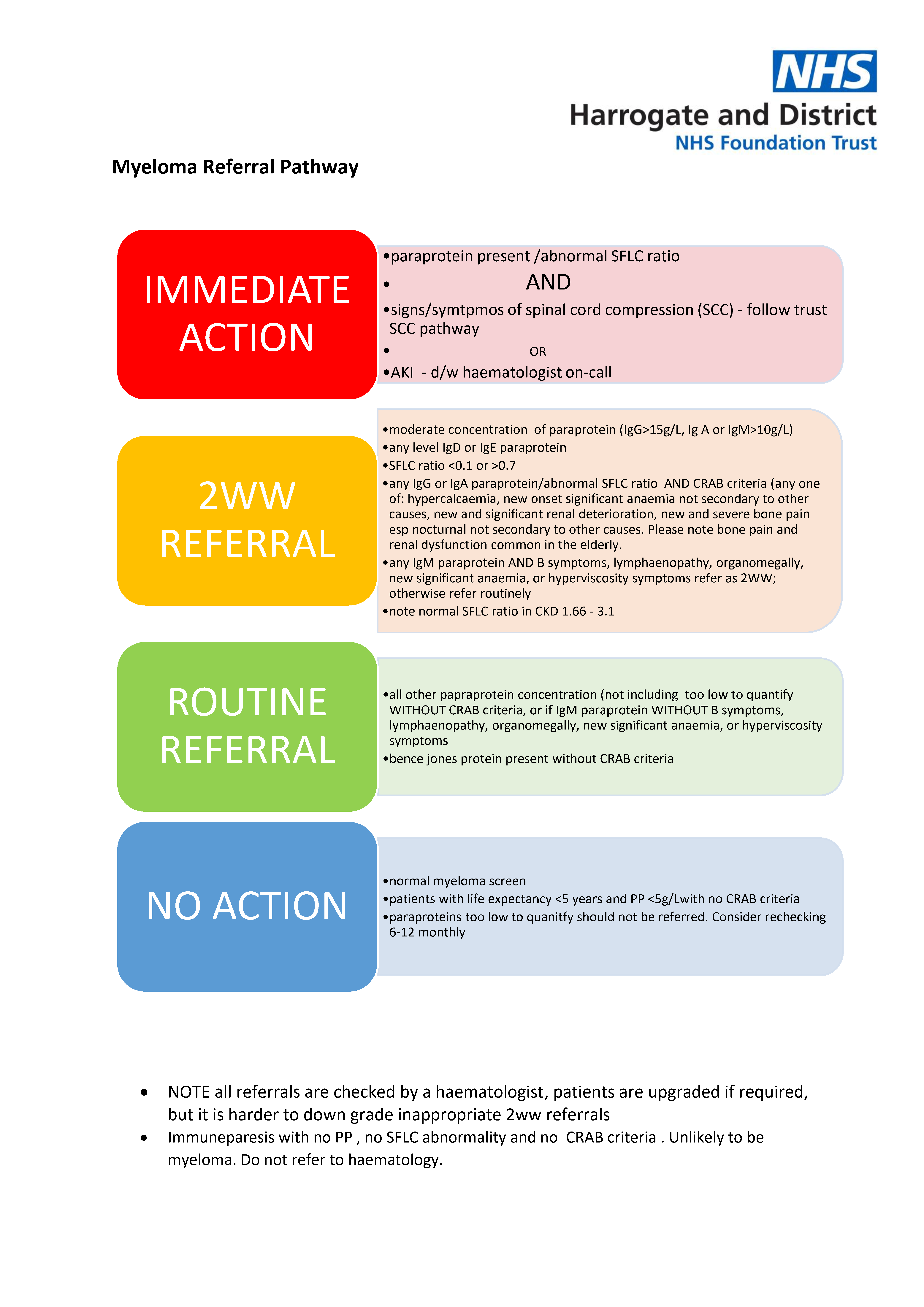
Immediate action if:
- Paraprotein present / abnormal SFLC ratio
AND - Signs / symptoms of spinal cord compression (SCC) - follow trust SCC pathway
OR - AKI - d/w haematologist on-call
USC referral if:
- moderate concentration of paraprotein (IgG>15g/L, Ig A or IgM>10g/L)
- any level IgD or IgE paraprotein
- SFLC ratio <0.1 or >0.7
- any IgG or IgA paraprotein/abnormal SFLC ratio AND CRAB criteria (any one of: hypercalcaemia, new onset significant anaemia not secondary to other causes, new and significant renal deterioration, new and severe bone pain esp nocturnal not secondary to other causes. Please note bone pain and renal dysfunction common in the elderly.
- any IgM paraprotein AND B symptoms, lymphaenopathy, organomegally, new significant anaemia, or hyperviscosity symptoms refer as 2WW; otherwise refer routinely
- note normal SFLC ratio in CKD 1.66 - 3.1
Routine referral if:
- all other papraprotein concentration (not including too low to quantify WITHOUT CRAB criteria, or if IgM paraprotein WITHOUT B symptoms, lymphaenopathy, organomegally, new significant anaemia, or hyperviscosity symptoms
- bence jones protein present without CRAB criteria
No action if:
- normal myeloma screen
- patients with life expectancy <5 years and PP <5g/Lwith no CRAB criteria
- paraproteins too low to quanitfy should not be referred. Consider rechecking 6-12 monthly
Additional Resources & Reference
Associated Policies
Places covered by
- North Yorkshire
Hospital Trusts
Harrogate and District