HNY Policy and Pathway Repository - North Yorkshire
Vitamin B12 deficiency
Definition/Description
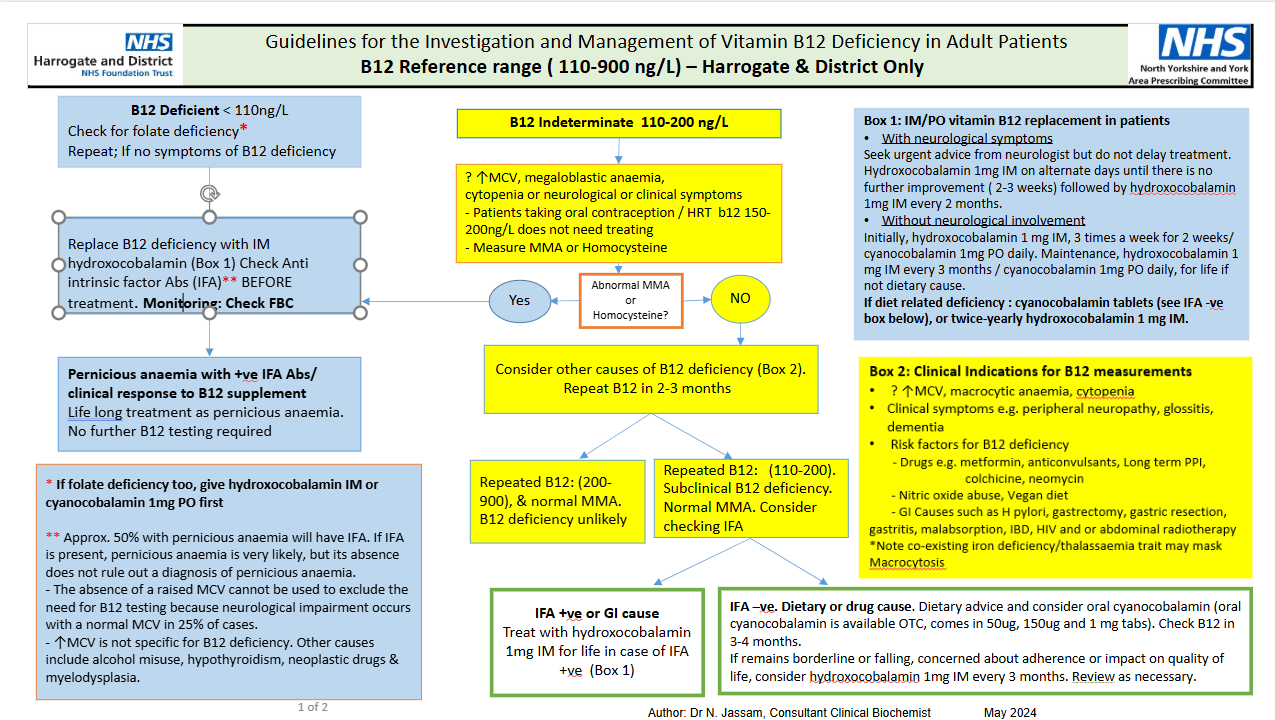
B12 Reference range (110–900 ng/L) – Harrogate & District Only
Red Flag Symptoms
- Seek urgent advice from a haematologist if the person has neurological symptoms, or is a pregnant woman.
- Haematologist/Biochemist if functional B12 deficiency is suspected i.e. strong clinical features of B12 deficiency, despite normal vitamin B12.
Guidelines on Management
B12 Deficient <110 ng/L
- Check for folate deficiency*
- Repeat: if no symptoms of B12 deficiency
- → Replace B12 deficiency with IM hydroxocobalamin (Box 1)
- Check Anti Intrinsic factor Abs (IFA)** BEFORE treatment.
- Monitoring: Check FBC
- Pernicious anaemia with ↑ve IFA Abs / clinical response to B12 supplement
- Life‑long treatment as pernicious anaemia.
- No further B12 testing required.
* If folate deficiency too, give hydroxocobalamin IM or cyanocobalamin 1mg PO first
** Approx. 50% with pernicious anaemia will have IFA. If IFA is present, pernicious anaemia is very likely, but its absence does not rule out a diagnosis of pernicious anaemia.
- The absence of a raised MCV cannot be used to exclude the need for B12 testing because neurological impairment occurs with a normal MCV in 25% of cases.
- ↑MCV is not specific for B12 deficiency. Other causes include alcohol misuse, hypothyroidism, neoplastic drugs & myelodysplasia.
B12 Indeterminate 110-200 ng/L
- ? ↑MCV, megaloblastic anaemia, cytopenia or neurological or clinical symptoms
- Patients taking oral contraception / HRT b12 150-200ng/L does not need treating
- Measure MMA or Homocysteine
- Abnormal MMA or Homocysteine?
- If Yes, then go to →
- If No then:
- Consider other causes of B12 deficiency (Box 2). Repeat B12 in 2-3 months:
- Repeated B12: (200-900), & normal MMA. B12 deficiency unlikely
- Repeated B12: (110-200). Subclinical B12 deficiency. Normal MMA. Consider checking IFA
- IFA +ve or GI cause - Treat with hydroxocobalamin 1mg IM for life in case of IFA +ve (Box 1)
- IFA –ve. Dietary or drug cause. Dietary advice and consider oral cyanocobalamin (oral cyanocobalamin is available OTC, comes in 50ug, 150ug and 1 mg tabs). Check B12 in 3-4 months.
If remains borderline or falling, concerned about adherence or impact on quality of life, consider hydroxocobalamin 1mg IM every 3 months. Review as necessary.
- Consider other causes of B12 deficiency (Box 2). Repeat B12 in 2-3 months:
- With neurological symptoms
- Seek urgent advice from neurologist but do not delay treatment. Hydroxocobalamin 1mg IM on alternate days until there is no further improvement ( 2-3 weeks) followed by hydroxocobalamin 1mg IM every 2 months.
- Without neurological involvement
- Initially, hydroxocobalamin 1 mg IM, 3 times a week for 2 weeks/ cyanocobalamin 1mg PO daily. Maintenance, hydroxocobalamin 1 mg IM every 3 months / cyanocobalamin 1mg PO daily, for life if not dietary cause.
- If diet related deficiency : cyanocobalamin tablets (see IFA -ve box below), or twice-yearly hydroxocobalamin 1 mg IM.
Box 2: Clinical Indications for B12 measurements
- ? ↑MCV, macrocytic anaemia, cytopenia
- Clinical symptoms e.g. peripheral neuropathy, glossitis, dementia
- Risk factors for B12 deficiency
- Drugs e.g. metformin, anticonvulsants, Long term PPI, colchicine, neomycin
- Nitric oxide abuse, Vegan diet
- GI Causes such as H pylori, gastrectomy, gastric resection, gastritis, malabsorption, IBD, HIV and or abdominal radiotherapy
* Note co-existing iron deficiency/thalassaemia trait may mask Macrocytosis
Referral Criteria/Information
Treatment of folate deficiency anaemia: Prescribe oral folic acid 5 mg daily — in most people, treatment will be required for 4 months. However, folic acid may need to be taken for longer (sometimes for life) if the underlying cause of deficiency is persistent.
Check vitamin B12 levels in all people before starting folic acid — treatment can improve well-being, mask underlying B12 deficiency, and allow neurological disease to develop.
Seek urgent advice:
Haematologist/Biochemist if functional B12 deficiency is suspected i.e. strong clinical features of B12 deficiency, despite normal vitamin B12.
Referral Advice for B12 or folate deficiency anaemia?
Refer to a Haematologist if:
- The cause of vitamin B12 or folate deficiency is uncertain, or unclear following investigations.
- Haematological malignancy or other blood disorder is suspected — refer urgently using a suspected cancer pathway referral (for an appointment within 2 weeks).
- The person does not respond to treatment.
- The mean cell volume is persistently greater than 100 femtolitres.
Refer to a Gastroenterologist if:
- Malabsorption or an inflammatory bowel disorder is suspected.
- The person has pernicious anaemia and gastrointestinal symptoms, especially if there is a suspicion of gastric cancer (for example co-existing iron deficiency).
- If gastric cancer is suspected, refer urgently using a suspected cancer pathway referral (for an appointment within 2 weeks).
Exceptions:
Pregnancy
- Use active B12 as the initial test for suspected vitamin B12 deficiency during pregnancy.
Recreational nitrous use
- Use total B12 & plasma homocysteine or serum MMA as the initial test in recreational nitrous use.
Additional Resources & Reference
Further Information
NICE guideline, NG239: Vitamin B12 deficiency in over 16s: diagnosis and management
OR/ and
NICE CKS: Management of anaemia - vitamin B12 and folate deficiency
Vitamin B12 replacement: ongoing care and follow up
Intrinsic factor tests for B12 deficiency
These have been taking to long to enable a good result, Dr Jassam has suggested if that the MMA test Methylmalonic acid is elevated - this can be used to as evidence of b12.
Associated Policies
Specialties
Places covered by
- North Yorkshire
Hospital Trusts
Harrogate and District