HNY Policy and Pathway Repository - North Yorkshire
Thrombocytopenia
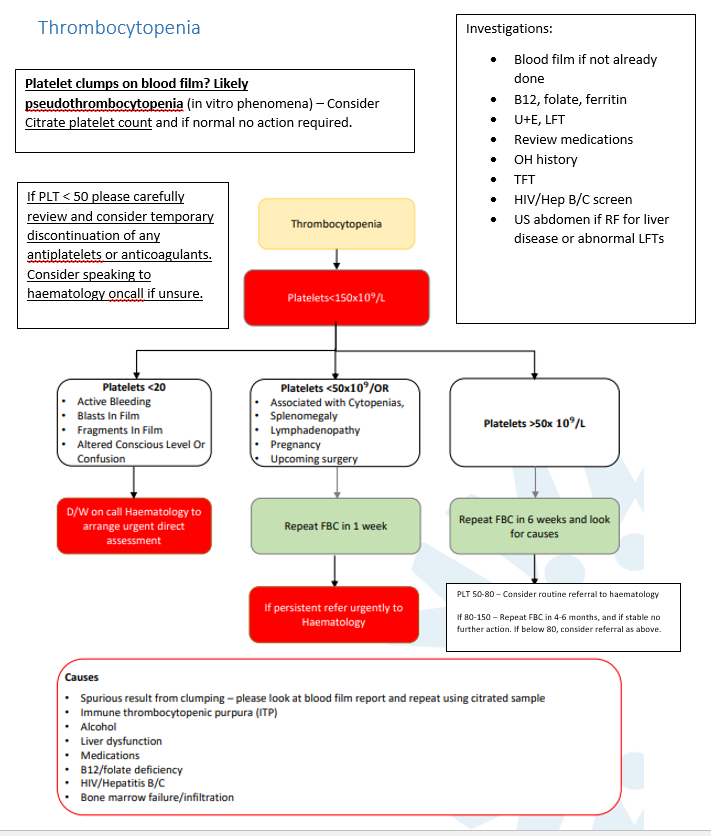
Definition/Description
Platelets < 150 ×10⁹/L
Red Flag Symptoms
Platelets < 20
- Active bleeding
- Blasts in film
- Fragments in film
- Altered conscious level or confusion
Guidelines on Management
If platelet clumps on blood film:
- Likely pseudothrombocytopenia (in vitro phenomenon)
- Consider Citrate platelet count and if normal no action required
If PLT < 50 please carefully review and consider temporary discontinuation of any antiplatelets or anticoagulants.
Consider speaking to haematology on call if unsure
Consider speaking to haematology on call if unsure
Causes
- Spurious result from clumping – please look at blood film report and repeat using citrated sample
- Immune thrombocytopenic purpura (ITP)
- Alcohol
- Liver dysfunction
- B12/folate deficiency
- HIV/hepatitis B/C
- Bone marrow failure/infiltration
Investigations:
- Blood film if not already done
- B12, folate, ferritin
- U+E, LFT
- Review medications
- OH history
- TFT
- HIV/Hep B/C screen
- US abdomen if RF for liver disease or abnormal LFTs
Referral Criteria/Information
D/W on call Haematology to arrange urgent direct assessment if:
- Platelets < 20
- Active bleeding
- Blasts in film
- Fragments in film
- Altered conscious level or confusion
Refer urgently to Haematology if:
- Platelets < 50 ×10⁹/L OR
- Associated with cytopenias
- Splenomegaly
- Lymphadenopathy
- Pregnancy
- Upcoming surgery
- Repeat FBC in 1 week - if persistent then urgent referral
Consider routine referral to haematology:
- Platelets > 50 ×10⁹/L
- Repeat FBC in 6 weeks and look for causes
- If PLT 50–80 then consider routine referral
-
If 80–150 → Repeat FBC in 4–6 months, and if stable no further action. If below 80, consider referral as above.
Associated Policies
There are no associated policies.
Specialties
Places covered by
- North Yorkshire
Hospital Trusts
Harrogate and District
Date created: 18/03/2026, 12:17
Last modified: 18/03/2026, 12:19
Date due for review: 18/03/2028