HNY Policy and Pathway Repository - North Yorkshire
Suspected myeloma
Definition/Description
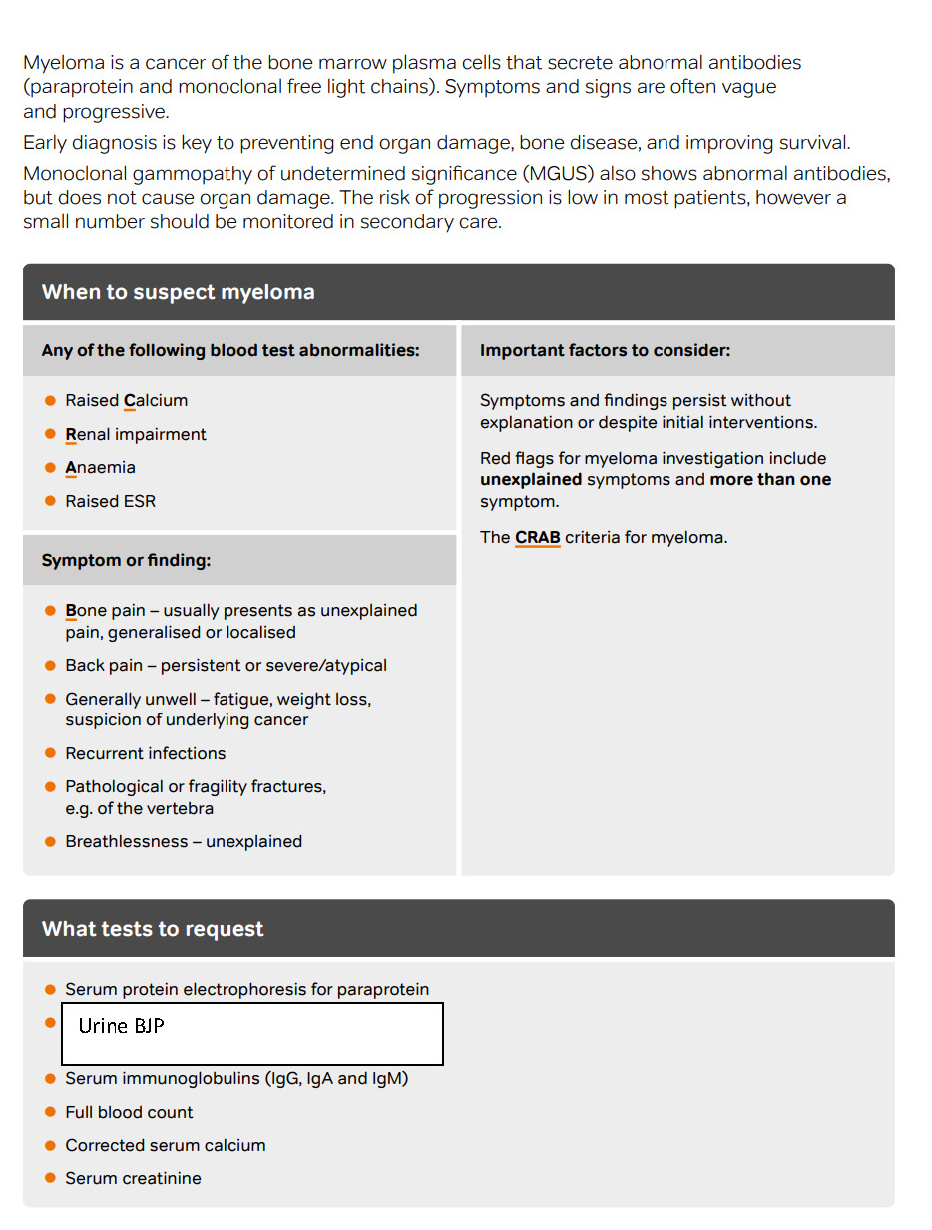
Myeloma is a cancer of the bone marrow plasma cells that secrete abnormal antibodies (paraprotein and monoclonal free light chains). Symptoms and signs are often vague and progressive.
Early diagnosis is key to preventing end organ damage, bone disease, and improving survival.
Monoclonal gammopathy of undetermined significance (MGUS) also shows abnormal antibodies, but does not cause organ damage. The risk of progression is low in most patients, however a small number should be monitored in secondary care.
Red Flag Symptoms
- Paraprotein present / abnormal sFLC ratio / BJP AND
- Signs/symptoms of spinal cord compression (SCC) – follow trust SCC pathway OR
- Significant AKI – D/W haematologist on‑call
Guidelines on Management
When to suspect myeloma?
Any of the following blood test abnormalities:
- Raised Calcium
- Renal impairment
- Anaemia
- Raised ESR
Symptom or finding:
- Bone pain – usually presents as unexplained pain, generalised or localised
- Back pain – persistent or severe/atypical
- Generally unwell – fatigue, weight loss, suspicion of underlying cancer
- Recurrent infections
- Pathological or fragility fractures, e.g. of the vertebra
- Breathlessness – unexplained
Important factors to consider:
Symptoms and findings persist without explanation or despite initial interventions.
Red flags for myeloma investigation include unexplained symptoms and more than one symptom.
The CRAB criteria for myeloma.
What tests to request
- Serum protein electrophoresis for paraprotein
- Urine BJP
- Serum immunoglobulins (IgG, IgA and IgM)
- Full blood count
- Corrected serum calcium
- Serum creatinine
Referral Criteria/Information
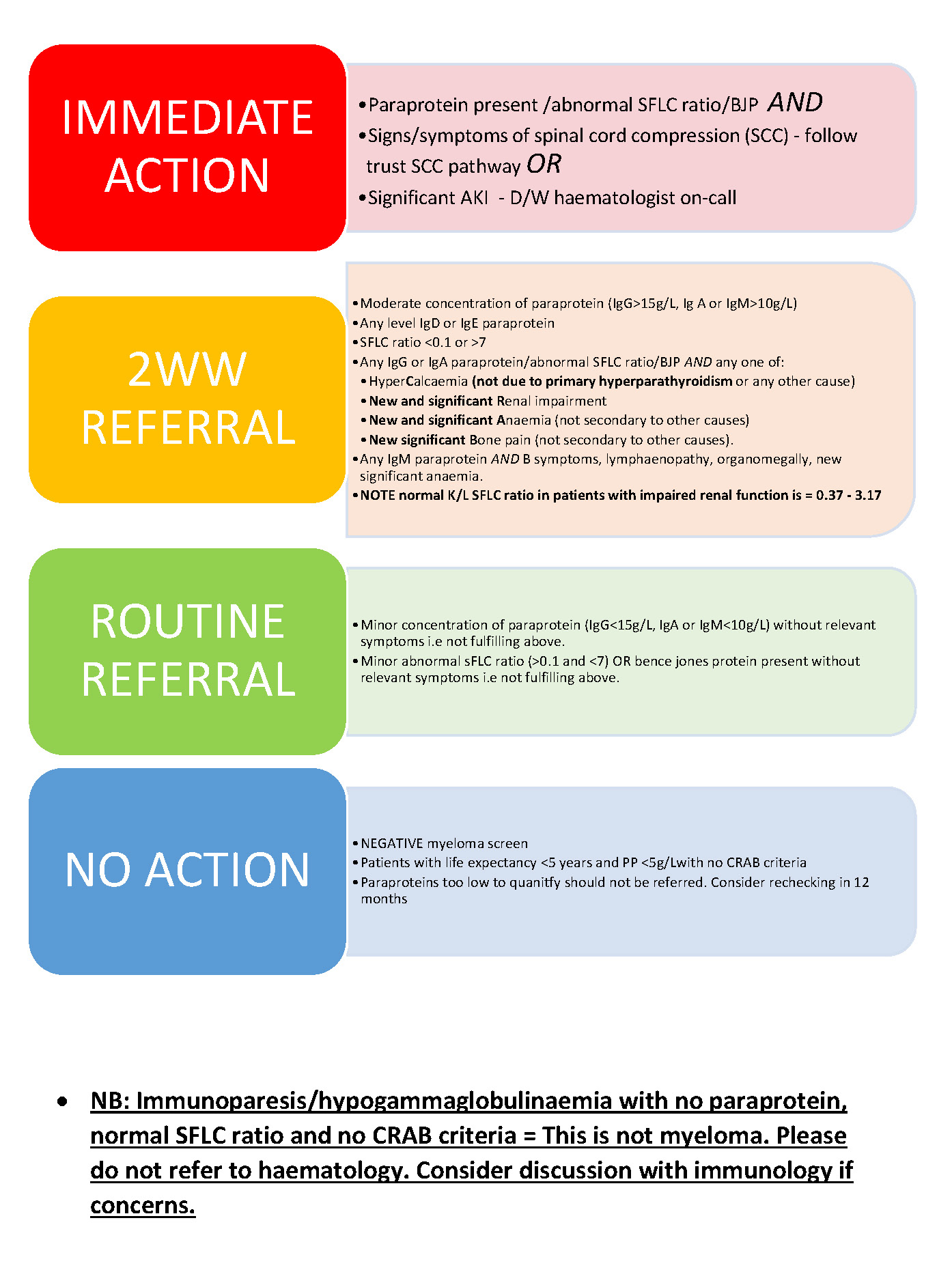
IMMEDIATE ACTION
- Paraprotein present / abnormal sFLC ratio / BJP AND
- Signs/symptoms of spinal cord compression (SCC) – follow trust SCC pathway OR
- Significant AKI – D/W haematologist on‑call
USC REFERRAL
- Moderate concentration of paraprotein (IgG >15 g/L, IgA or IgM >10 g/L)
- Any IgD or IgE paraprotein
- sFLC ratio <0.1 or >7
- ANY of: paraprotein/abnormal sFLC ratio/BJP AND any one of:
- Hypercalcaemia (not due to primary hyperparathyroidism or any other cause)
- New and significant Renal impairment
- New and significant Anaemia (not secondary to other causes)
- New significant Bone pain (not secondary to other causes)
- Any IgM paraprotein AND B symptoms, lymphadenopathy, organomegaly, new significant anaemia
- NOTE: Normal κ/λ sFLC ratio in patients with impaired renal function is 0.37 – 3.17
ROUTINE REFERRAL
- Minor concentrations of paraprotein (IgG ≤15 g/L, IgA or IgM ≤10 g/L) without relevant symptoms i.e., not fulfilling above.
- Minor abnormal sFLC ratio (0.1–7) OR Bence Jones protein present without relevant symptoms i.e., not fulfilling above.
NO ACTION
- NEGATIVE myeloma screen
- Patients with life expectancy <5 years and PP <5 g/L with no CRAB criteria
- Paraproteins too low to quantify should not be referred. Consider rechecking in 12 months.
Additional Resources & Reference
Associated Policies
Specialties
Places covered by
- North Yorkshire
Hospital Trusts
Harrogate and District