HNY Policy and Pathway Repository - North Yorkshire
Suspected lower GI / colorectal cancer
Definition/Description
Suspected GI / colorectal cancer
Red Flag Symptoms
None provided
Guidelines on Management
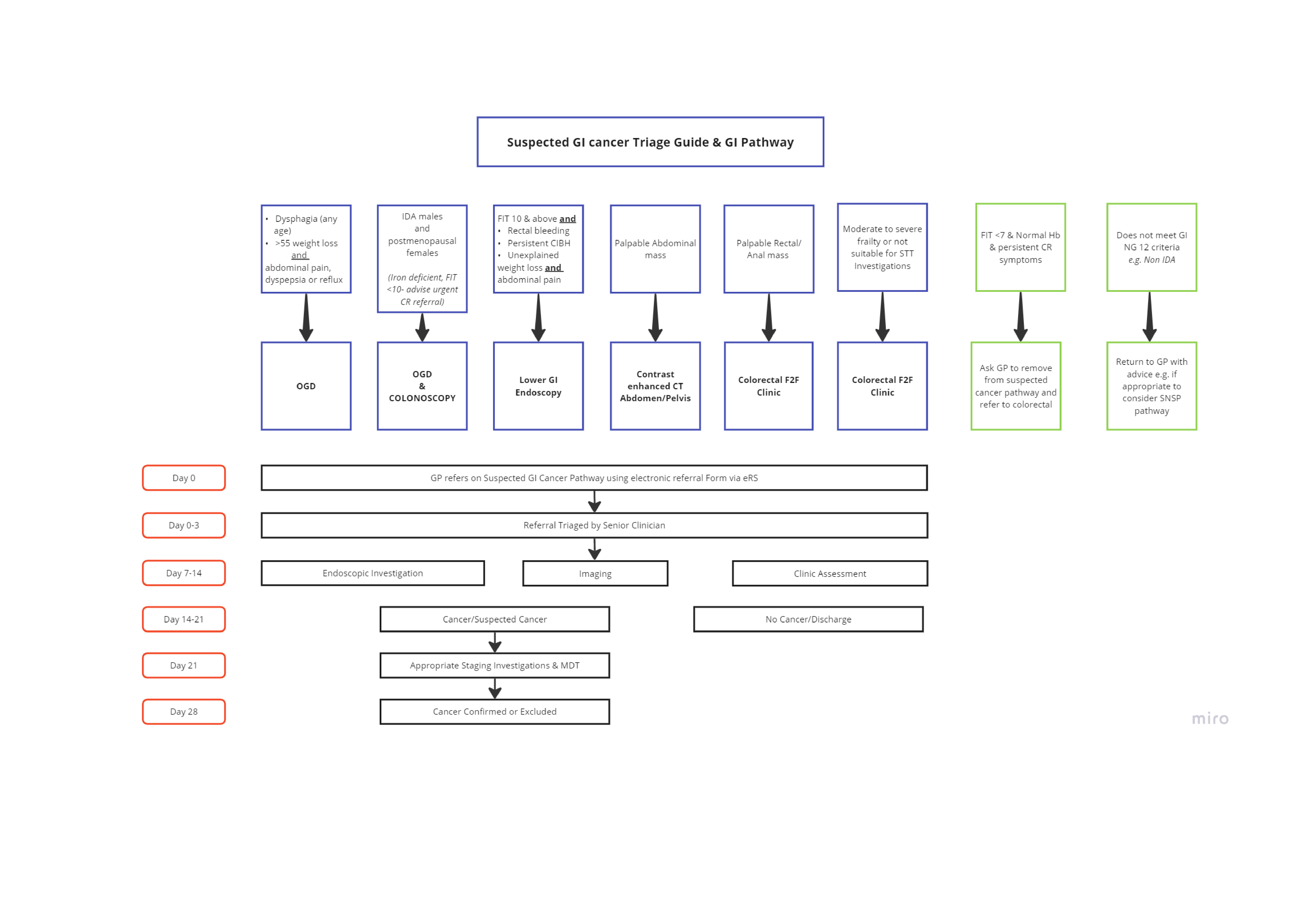
OGD if
- Dysphagia (any age)
- >55 weight loss AND abdominal pain, dyspepsia or reflux
OGD and colonoscopy if
- IDA male
OR - Post-menopausal female
(Iron deficient, FIT <10 - advise urgent CR referral)
Lower GI endoscopy if
FIT 10 & above AND:
- Rectal bleeding
- Persistent CIBH
- Unexplained weight loss AND abdominal pain
Contrast enhanced CT abdomen / pelvis if
- Palpable abdominal mass
Colorectal F2F clinic if
- Palpable rectal anal mass
AND/OR - Moderate to severe frailty or not suitable for STT investigations
(See also colorectal pathway information below)
Ask GP to remove from suspected cancer pathway and refer to colorectal if
Return to GP with advice if
(If appropriate, consider SNSP pathway) |
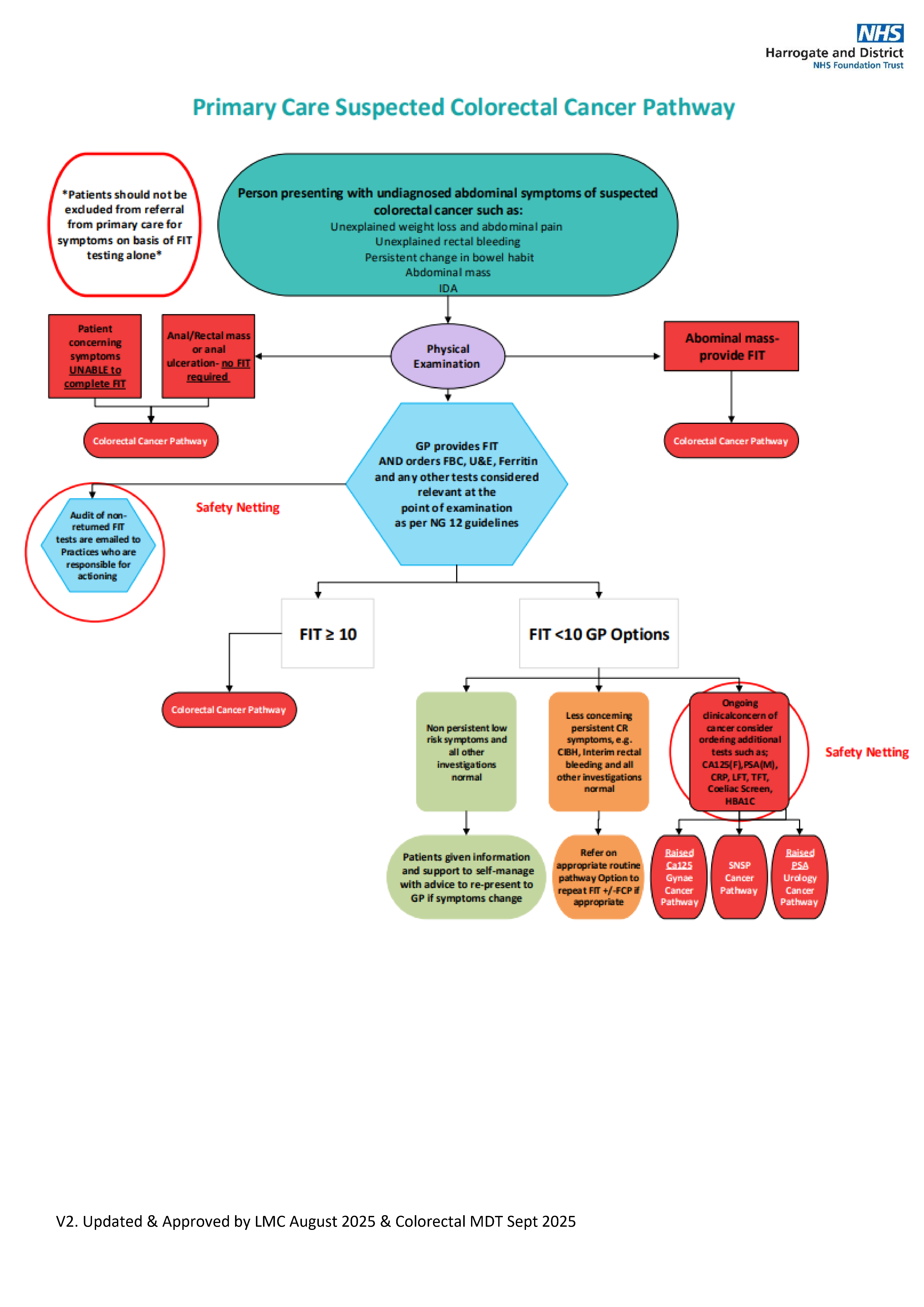
Colorectal cancer pathway
Person presenting with undiagnosed abdominal symptoms of suspected coloractal cancer such as:
- Unexplained weigh loss and abdominal pain
- Unexplained rectal bleeding
- Persistent change in bowel habit
- Abdominal mass
- IDA
After physical examination refer via colorectal cancer pathway if:
- Abdominal mass found (provide FIT)
- Anal / rectal mass or anal ulceration (no FIT required)
- Patient concerning symptoms (unable to complete RT)
GP to provide FIT AND orders FBC, U&E, Ferritin and any other tests considered relevant at the point of examination as per NG12 guidelines:
Colorectal cancer pathway if:
- FIT ≥ 10
If FIT <10 then options are:
- If has non-persistent low risk symptoms and all other investigations normal
- Give patient information and support to self manage with advice to re-present to GP if symptoms change:
- If has less concerning persistent CR symptoms (e.g. CIBH, interim rectal bleeding and all other investigations normal
- Refer on to appropriate routine pathway option to repeat FIT +/- FCP if appropriate
- If still has clinical concen of cancer, consider ordering additional tests such as CA125(F), PAS(M), CRP, LFT, TFT, coeliac screen, HbA1C (Safety Netting)
- Raised CA125 - gynae cancer pathway
- Raised PSA - urology cancer pathway
- SNSP cancer pathway
Referral Criteria/Information
Expected timeline for lower GI cancer pathway
- Day 0: GP refers on suspected GI cancer pathway using electronic referral form (via e-RS)
- Day 0-3: Referral triaged by senior clinican
- Day 7-14:
- Endoscopic investigation
- Imaging
- Clinic assessment
- Day 14-21: Assessed as either -
- Cancer / suspected cancer
- No cancer - discharged
- Day 21: Appropriate staging investigations & MDT
- Day 28: Cancer confirmed or excluded
Associated Policies
There are no associated policies.
Places covered by
- North Yorkshire
Hospital Trusts
Harrogate and District
Date created: 04/03/2026, 10:27
Last modified: 04/03/2026, 14:09
Date due for review: 04/03/2027