HNY Policy and Pathway Repository - North Yorkshire
Raised ferritin
Definition/Description
Raised ferritin:
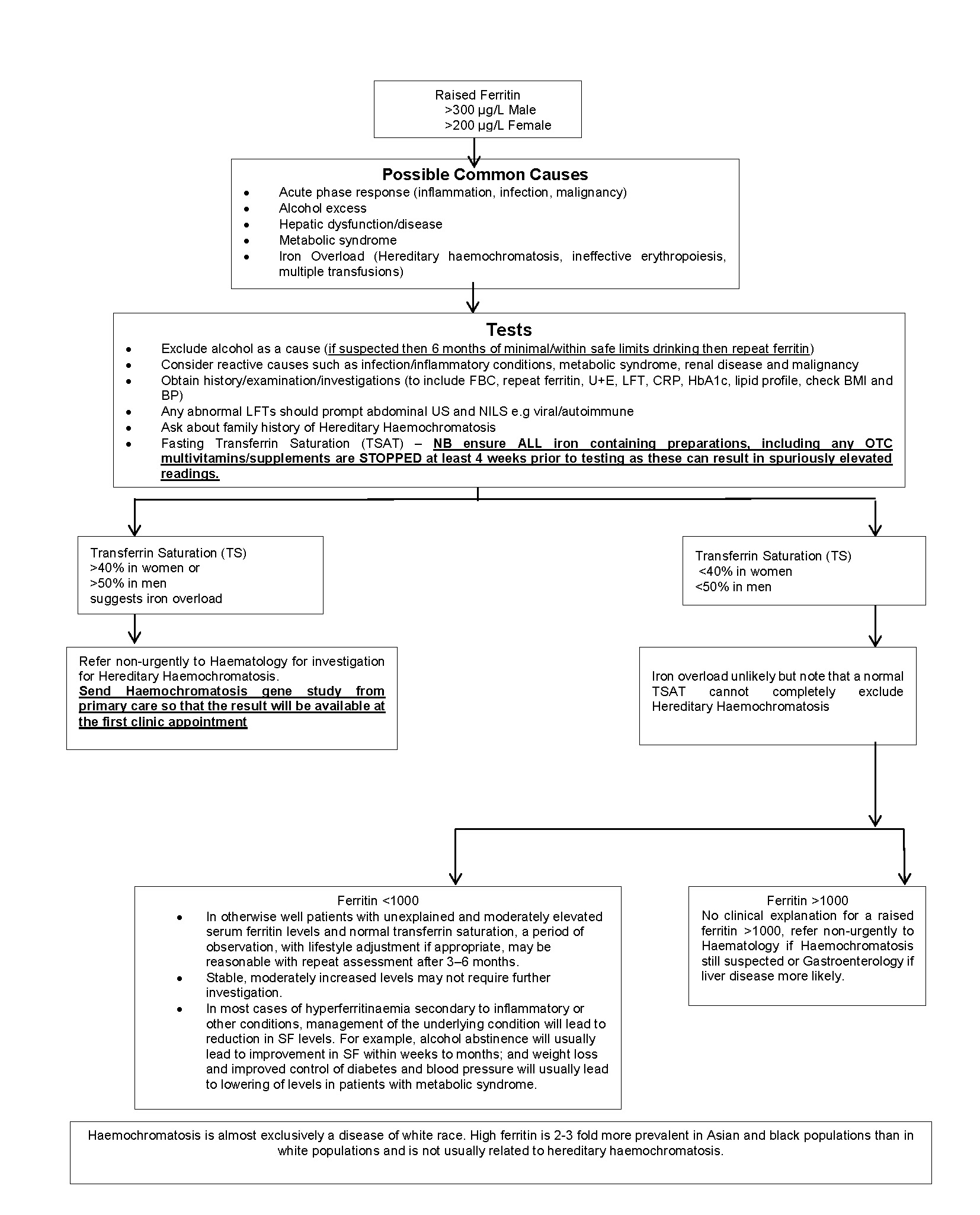
- Male: >300 µg/L
- Female: >200 µg/L
Red Flag Symptoms
None provided
Guidelines on Management
Possible common causes
- Acute phase response (inflammation, infection, malignancy)
- Alcohol excess
- Hepatic dysfunction / disease
- Metabolic syndrome
- Iron overload (hereditary haemochromatosis, ineffective erythropoisis, multiple transfusions)
Tests
- Exclude alcohol as a cause (if suspected then 6 months of minimal/within safe limits drinking then repeat ferritin)
- Consider reactive causes such as infection/inflammatory conditions, metabolic syndrome, renal disease and malignancy
- Obtain history/examination/investigations (to include FBC, repeat ferritin, U+E, LFT, CRP, HbA1c, lipid profile, check BMI and BP)
- Any abnormal LFTs should prompt abdominal US and NILS e.g. viral/autoimmune
- Ask about family history of Hereditary Haemochromatosis
- Fasting Transferrin Saturation (TSAT) — NB ensure ALL iron‑containing preparations, including any OTC multivitamins/supplements, are STOPPED at least 4 weeks prior to testing as these can result in spuriously elevated readings.
Haemochromatosis is almost exclusively a disease of white race. High ferritin is 2–3 fold more prevalent in Asian and black populations than in white populations and is not usually related to hereditary haemochromatosis.
Referral Criteria/Information
Routine referal to haematology for investigation for Hereditary Haemochromatosis if:
- Transferrin Saturation (TS) suggests iron overload:
- >40% in women
or - >50% in men
- >40% in women
- Send Haemochromatosis gene study from primary care so that the result will be available at the first clinic appointment
Iron overload unlikely, but note that a normal TSAT cannot completely exclude Hereditary Haemochromatosis if:
- Transferrin Saturation (TS)
- <40% in women
or - <50% in men
- <40% in women
Ferritin <1000
- In otherwise well patients with unexplained and moderately elevated serum ferritin levels and normal transferrin saturation, a period of observation, with lifestyle adjustment if appropriate, may be reasonable with repeat assessment after 3–6 months.
- Stable, moderately increased levels may not require further investigation.
- In most cases of hyperferritinaemia secondary to inflammatory or other conditions, management of the underlying condition will lead to reduction in SF levels. For example, alcohol abstinence will usually lead to improvement in SF within weeks to months; and weight loss and improved control of diabetes and blood pressure will usually lead to lowering of levels in patients with metabolic syndrome.
Ferritin >1000
No clinical explanation for a raised ferritin >1000:
Refer non‑urgently to Haematology if Haemochromatosis still suspected, or Gastroenterology if liver disease more likely.
Associated Policies
There are no associated policies.
Specialties
Places covered by
- North Yorkshire
Hospital Trusts
Harrogate and District
Date created: 18/03/2026, 11:43
Last modified: 18/03/2026, 11:43
Date due for review: 18/03/2028