HNY Policy and Pathway Repository - North Yorkshire
Neutropenia
Definition/Description
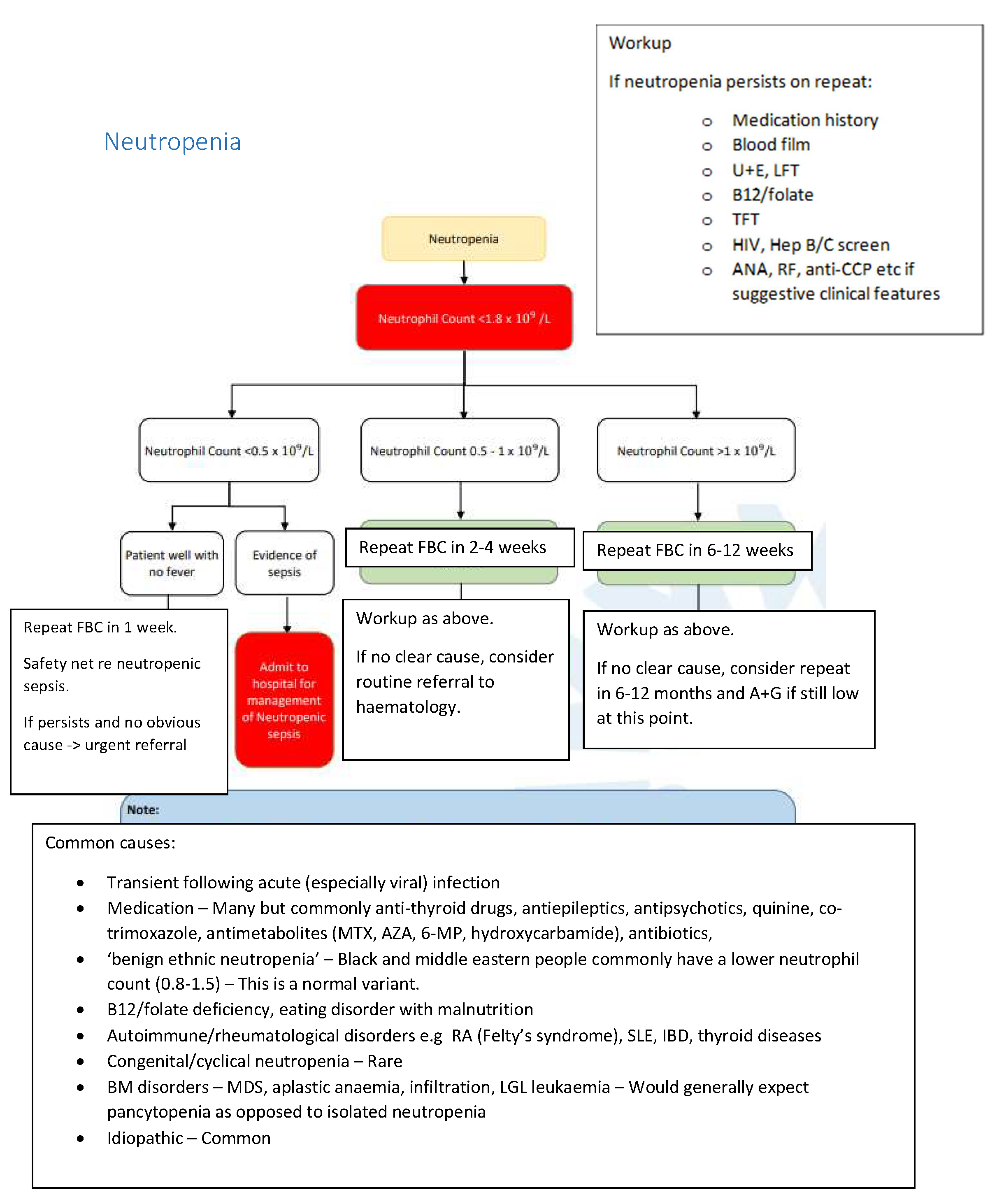
Neutrophil count <1.8 x 109/L
Red Flag Symptoms
None provided
Guidelines on Management
Common causes
- Transient following acute (especially viral) infections
- Medication - many but commonly anti-thyroid drugs, antiepileptics, antipsychotics, quinine, co-trimoxazole, antimetabolites (MTX, AZA, 6-MP, hydroxycarbamide), antibiotics
- "Benign ethinic neutropenia" - Black and middle eastern people commonly have a lower neutrophil count (0.8-1.5) - this is a normal variant.
- B12 / folate deficiency, eating disorder with malnutrition
- Authoimmune / rheumatological disorders e.g. RA (Felty's syndrome), SLE, IBD, thyroid diseases
- Congenital / cyclical neutropenia - rare
- BM disorders - MDS, aplastic anaemia, infiltration, LGL leukarmia - would generally expect pancytopenia as opposed to isolated neutropenia
- Idiopathic - common
Workup
If neutropenia persists on repeat:
- Medication history
- Blood film
- U+E, LFT
- B12 / folate
- TFT
- HIV, Hep B/C screen
- ANA, RF, anti-CCP ect if suggestive clinical features
Referral Criteria/Information
Urgent referral
- Neutrophil count <0.5 x 109/L
- Patient well with no fever
- Repeat FBC in 1 week
- Safety net RE: neutropenic sepsis
- If persists and no obvious cause then urgent referral
Admit to hospital for management of Neutropenic sepsis if:
- Neutrophil count <0.5 x 109/L
- Evidence of sepsis
Consider routine referral to haematology if:
- Neutrophil count 0.5 - 1 x 109/L
- Repeat FBC in 2-4 weeks
- Workup (see "guidelines on management" section)
- If no clear cause, consider routine referral to haematology
Consider A&G if:
- Neutrophil count >1 x 109/L
- Repeat FBC in 6-12 weeks
- Workup (see "guidelines on management" section)
- If no clear cause, consider repeat in 6-12 months and A&G if still low at this point.
Associated Policies
There are no associated policies.
Specialties
Places covered by
- North Yorkshire
Hospital Trusts
Harrogate and District
Date created: 18/03/2026, 10:34
Last modified: 18/03/2026, 10:34
Date due for review: 18/03/2028