HNY Policy and Pathway Repository - North Yorkshire
Microcytic anaemia
Definition/Description
Microcytic anaemia, with low MCV and/or MCH.
Definition of anaemia:
Adult male |
Haemoglobin <130g/l |
Non-pregnant adult female |
Haemoglobin <120g/l |
Children |
Haemoglobin below age -and gender- specific reference range |
Red Flag Symptoms
None provided
Guidelines on Management
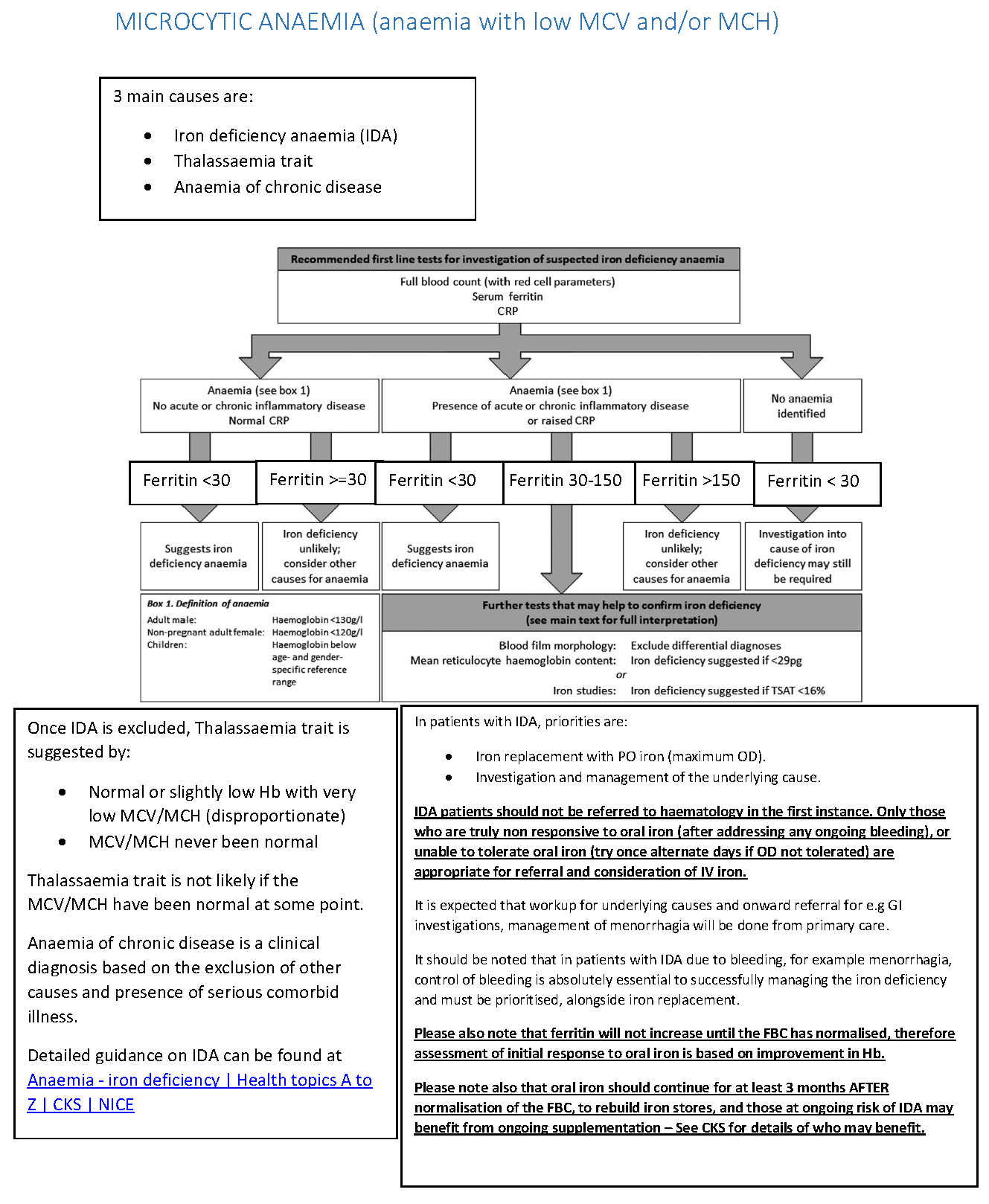
Main causes
- Iron deficiency anaemia (IDA)
- Thalassaemia trait
- Anaemia of chronic disease
Recommended first line tests for investigation of suspected iron deficiency anaemia
- Full blood count (with red cell parameters)
- Serum ferritin
- CRP
Anaemia - no acute or chronic inflammatory disease, normal CRP
- Ferritin <30
- Suggests iron deficienct anaemia
- Ferritin >=30
- Iron deficiency unlikely; consider other causes for anaemia
Anaemia - presence of acute or chronic inflammatory disease or raised CRP
- Ferritin <30
- Suggests iron deficiency anaemia
- Ferritin 30-150
- Further tests that may help to confirm iron deficiency:
- Blood film morphology: exclude differential diagnoses
- Mean reticulocyte haemoglobin content: iron deficiency suggested if <29pg
or - Iron studies: iron deficiency suggested if TSAT <16%
- Further tests that may help to confirm iron deficiency:
- Ferritin >150
- Iron deficiency unlikely; consider other causes for anaemia
No anaemia identified
- Ferritin <30
- Investigation into cause of iron deficiency may still be required
- Investigation into cause of iron deficiency may still be required
Once IDA is excluded, Thalassaemia trait is suggested by:
- Normal or slightly low Hb with very low MCV/MCH (disproportionate)
- MCV/MCH never been normal
Thalassaemia trait is not likely if the MCV/MCH have been normal at some point.
Anaemia chronic disease is a clinical diagnosis based on the exclusion of other causes and presence of serious comorbid illness.
Detailed guiance of IDA can be found at: https://cks.nice.org.uk/topics/anaemia-iron-deficiency/
Referral Criteria/Information
In patients with IDA, priorities are:
- Iron replacement with PO iron (maximum OD)
- Investigation and management of the underlying cause
IDA patients should not be referred to haematology in the first instance. Only those who are truly non-responses to oral iron (after addressing any ongoing bleeding), or unable to tolerate oral iron (try once alternate dates if OD not tolerated) are appropriate for referral and consideration of IV iron.
It is expected that workup for underlying causes and onward referral for e.g. GI investigations, management of menorrhaia will be done from primary care.
It should be noted that in patients with IDA due to bleeding, for example menorrhagia, control of bleeding is absolutely essential to successfully managing the iron deficiency and must be prioritied, along iron replacement.
Please also note that ferritin will not increase until the FBC has normalised, therefore assessment of initial response to oral irona is based on improvement in Hb.
Please note also that oral iron should continue for at lease 3 months AFTER normalisation of the FBC, to rebuild iron stores, and those at ongoing risk of IDA may benefit from ongoing supplementation - See CKS for details of who may benefit.
Associated Policies
Specialties
Places covered by
- North Yorkshire
Hospital Trusts
Harrogate and District