HNY Policy and Pathway Repository - North Yorkshire
High ferritin
Definition/Description
In healthy subjects the serum ferritin concentration correlates with iron stores, however high levels do not necessarily reflect iron overload. Ferritin behaves as an acute phase reactant in many inflammatory diseases. Tissue damage, particularly to the liver, can release large amounts of ferritin into the plasma.
Red Flag Symptoms
None provided
Guidelines on Management
Differential diagnosis:
- Acute phase reaction - infection, inflammation or malignancy.
- Release of ferritin by tissue damage, especially to iron rich organs - e.g. chronic liver disease (including alcoholic liver disease and cirrhosis) or splenic infarction.
- True iron overload - genetic haemochromatosis, iron overload secondary to repeated blood transfusions, massive ineffective erythropoeisis (thalassaemia, sideroblastic anaemia), porphyria cutanea tarda or rare genetic causes of iron overload.
Baseline investigations:
- FBC, LFT, CRP, iron studies (in particular fasting transferrin saturation). Repeat serum ferritin levels >3 months apart. If the fasting transferrin saturation is normal then this strongly suggests a falsely elevated ferritin rather than true iron overload.
- Genetic screening for haemochromatosis is indicated if positive family history OR if persistently raised ferritin with high transferrin saturation.
- If persistently raised ferritin with raised CRP and / or normal transferrin saturation then consider alternate causes.
Referral Criteria/Information
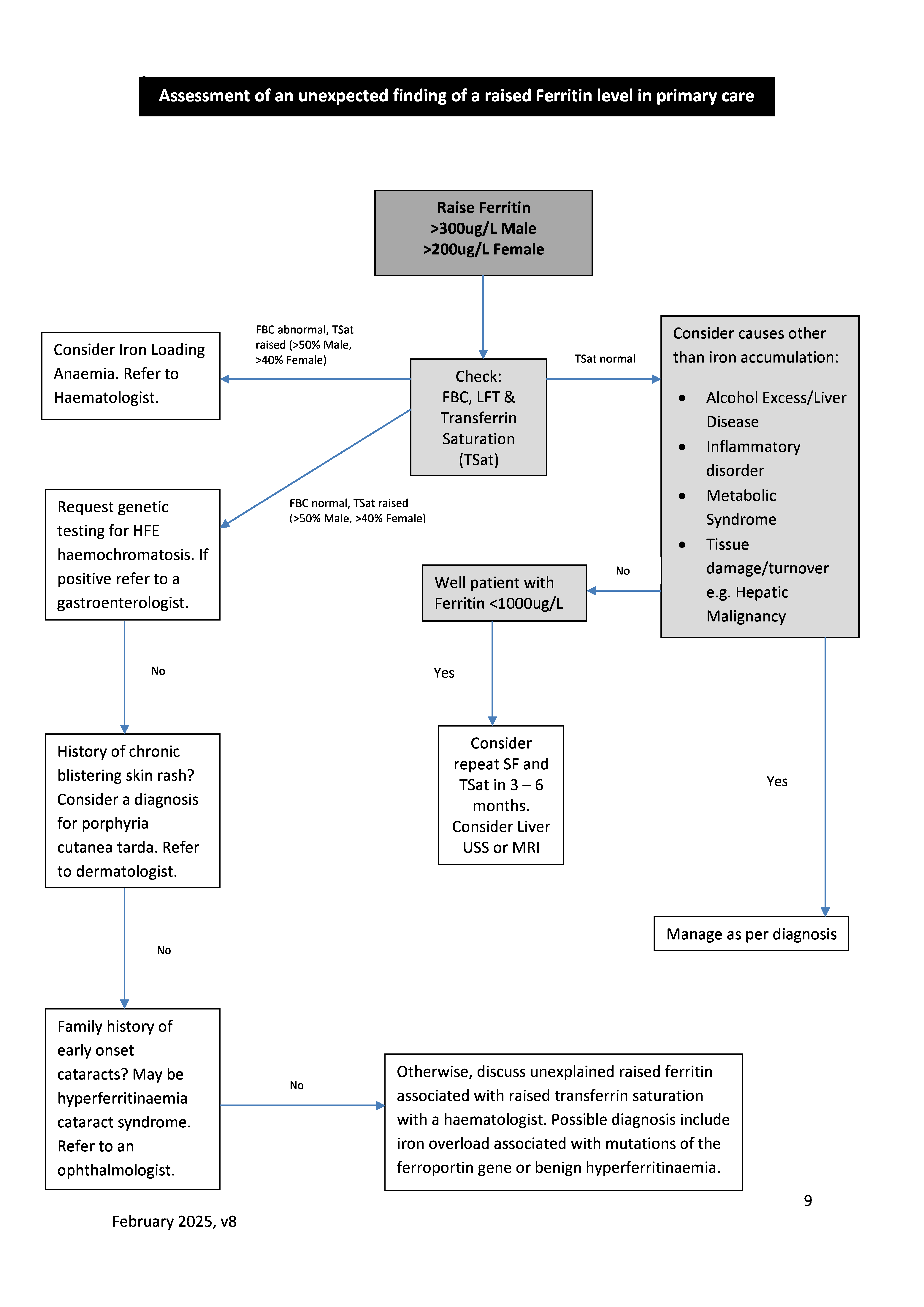
Referral (see flowchart below):
- If genetic haemochromatosis confirmed then patient management is usually overseen by Gastroenterology, although venesections are undertaken by Haematology. A referral to Gastroenterology would also be appropriate in patients found to have suspected liver disease on investigation of a high ferritin value.
- If family screening is required for genetic haemochromatosis (parents, siblings, children) then this can be undertaken in General Practice. Screening includes ferritin, transferrin saturation and possibly genetic studies. If genetic counselling is required then we suggest referral to the Clinical Genetics service.
- For raised serum ferritin associated with an acute phase response then the underlying condition may require further investigation and management.
- Refer to Haematology if true iron overload (raised ferritin and transferrin saturation) with uncertain cause (e.g. negative tests for genetic haemochromatosis) or known haemochromatosis to commence venesection.
Additional Resources & Reference
Haematology Handbook - South Tees Hospitals NHS Foundation Trust
References
Cullis JO, Fitzsimmons EJ, et al. Investigation and management of a raised serum ferritin. Br J Haematol 2018; 181: 331-340
Fitzsimmons EJ, Cullis JO, et al. Diagnosis and therapy of genetic haemochromatosis (review and 2017 update). Br J Haematol 2018; 181: 293 303
Associated Policies
There are no associated policies.
Specialties
Places covered by
- North Yorkshire
Hospital Trusts
South Tees Hospitals
Date created: 10/03/2026, 13:55
Last modified: 10/03/2026, 13:57
Date due for review: 01/02/2027