HNY Policy and Pathway Repository - Humber
Pulmonary Rehabilitation
Definition/Description
Robust evidence has repeatedly demonstrated improved exercise capacity and health related quality of life measures including decreased breathlessness, fatigue and healthcare utilisation for patients following a Pulmonary Rehabilitation (PR). In 2015 the Cochrane Airways Board made a decision to no longer update reviews comparing pulmonary rehabilitation to conventional intervention due to consistent beneficial findings (Lacasse et al., 2015).
This protocol has been reviewed and updated in line with British Thoracic Society (BTS) PR Guidelines (Bolton et al, 2013) and BTS Quality Standards for PR (BTS, 2014), the NICE COPD Guidance and quality standards and the National Respiratory Audit Programme (NRAP).
To ensure all staff and students operating within the Pulmonary Rehabilitation Team follow the correct processes and clinical procedure outlined within this Standard Operating Procedure.
Aims and Scope
The aims of this standard operating procedure for the Pulmonary Rehabilitation Team are as follows:
- Patients will be offered PR with a Medical Research Council (MRC) Dyspnoea score 3-5. Patients who are MRC dyspnoea score of 2 who are functionally limited by breathlessness (BTS 2014).
- Patients with MRC 1/2 to be offered PROMOTE.
- It is recommended that all standard PR patients are offered a place within 3 months of receipt of referral.
- For all patients referred for Early Rehabilitation (ER) (Post Discharge Fast Track) to be contacted and offered home or clinic appointment within 48- 72-hours of being discharged if on a Friday.
- It is recommended that patients hospitalised for acute exacerbation of COPD (ER patients), should be offered pulmonary rehabilitation at hospital discharge and to commence within 30 days of receipt of referral.
- To ensure a firm diagnosis has been obtained and the patient has no contraindications for and is motivated for the Pulmonary Rehabilitation Programme.
- Pulmonary rehabilitation is offered to individuals with a variety of respiratory conditions other than COPD that effect activities of daily living, such as Bronchiectasis, Interstitial lung disease (ILD), Lung surgery pre and post, Lung Cancer and Asthma, however, respiratory consultant MUST refer Asthma patients.
- National NHS England ratio for pulmonary rehabilitation provisions is 1:8. However, due to the early rehabilitation, complex, oxygen and long-covid patients attending pulmonary rehabilitation groups, we do recommend a minimum 1:4 staff ratio, this will further increase if patients require 1:1.
Red Flag Symptoms
Absolute Contraindications to Pulmonary Rehabilitation
- Unstable Angina
- Recent MI <6/52
- Recent CVA <6/52. TIA precautionary, must be medically optimised
- Unstable/Uncontrolled Arrhythmia
- Uncontrolled Epilepsy
- AAA>5.5 cm - require consultant/GP clearance (no resistance training)
- Acute +/or unstable left ventricular failure (LVF) and Cor-Pulmonale
- BMI of 16 or less
- Severe or uncontrolled tachycardia over 120 bpm
- Resting BP _> 180 Systolic
- Musculoskeletal or neurological condition which will limit patients’ ability to exercise e.g. Severe OA or peripheral vascular disease
- Patients who have significant cognitive or psychiatric impairment that would lead to the inability to follow simple commands in a group setting
Guidelines on Management
Home Rehabilitation Process
Following the triage process or following pre-assessment, it is determined by clinician or the referrer requesting a home assessment that the patient is more appropriate for home rehabilitation and is placed on home visit caseload.
Home rehabilitation can be offered during pre-assessment clinic if this intervention is more appropriate, or if the patient has a preference over group settings.
- A Clinician or appropriate Technical Instructor to review home visit caseload and arrange home visit.
- Completed initial assessment either therapy assessment sheet or technical instructor.
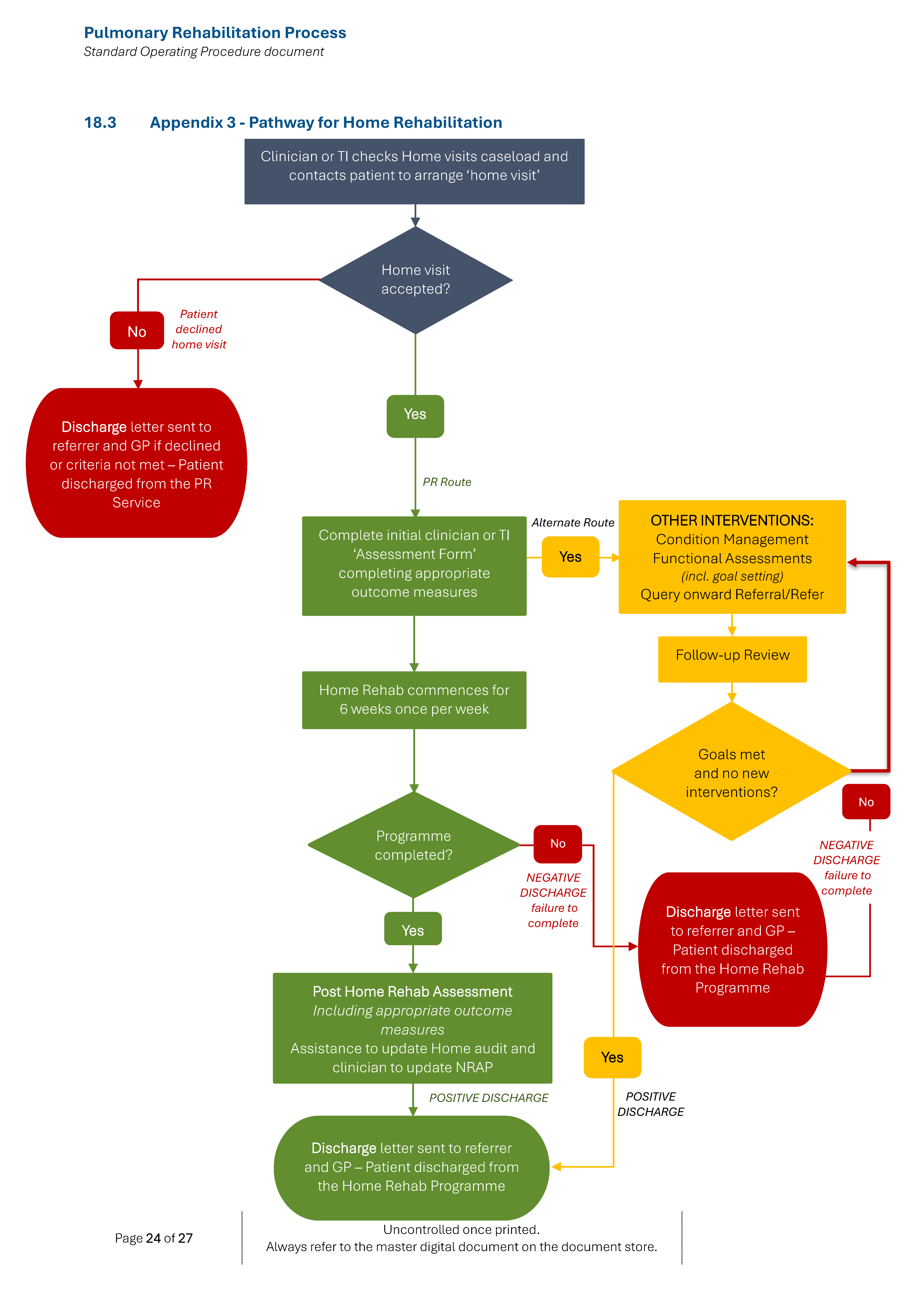
- Home rehabilitation consists of 6 weeks, x1 weekly supervised visit and expected x1 unsupervised exercise session.
- Discuss and document disclaimer.
- Complete Pre outcome measures at home: Standard list: Sit to stands in 1 minute, CAT score (COPD patients), HAD score and EQ-5D-5L. Other outcome measures can be added if clinically appropriate, such as grip and quadricep strength (using dynamometer if appropriate), SPPB.
- Outcome measures and field walk test: ISWT can be completed at the Centre if patients prefer to attend.
- Home sessions are individually tailored from the problem list and patient goals.
- Education to include topics covered in face-to-face PR program, via QR codes/YouTube/ written copies, handouts and staff delivery.
- Exercise diary to check unsupervised sessions.
- Discuss appropriate sign posting /onward referrals.
- Complete post-outcome measures (standardised as pre).
- Assessment and issuing of equipment if appropriate and patient engaging with home rehabilitation. If the patient is not appropriate for home rehab or declines input, onward referral to community therapy if equipment needs identified, unless unsafe and walking aid required.
- Identify if OT input required.
- Goals reviewed and achieved?
- Encouragement for long term lifestyle change and community exercise classes.
- Discharge letter summary to GP and discharge from service.
- To be included in NRAP data and details to be added to relevant list.
Please refer to Appendix 3 for pathway.
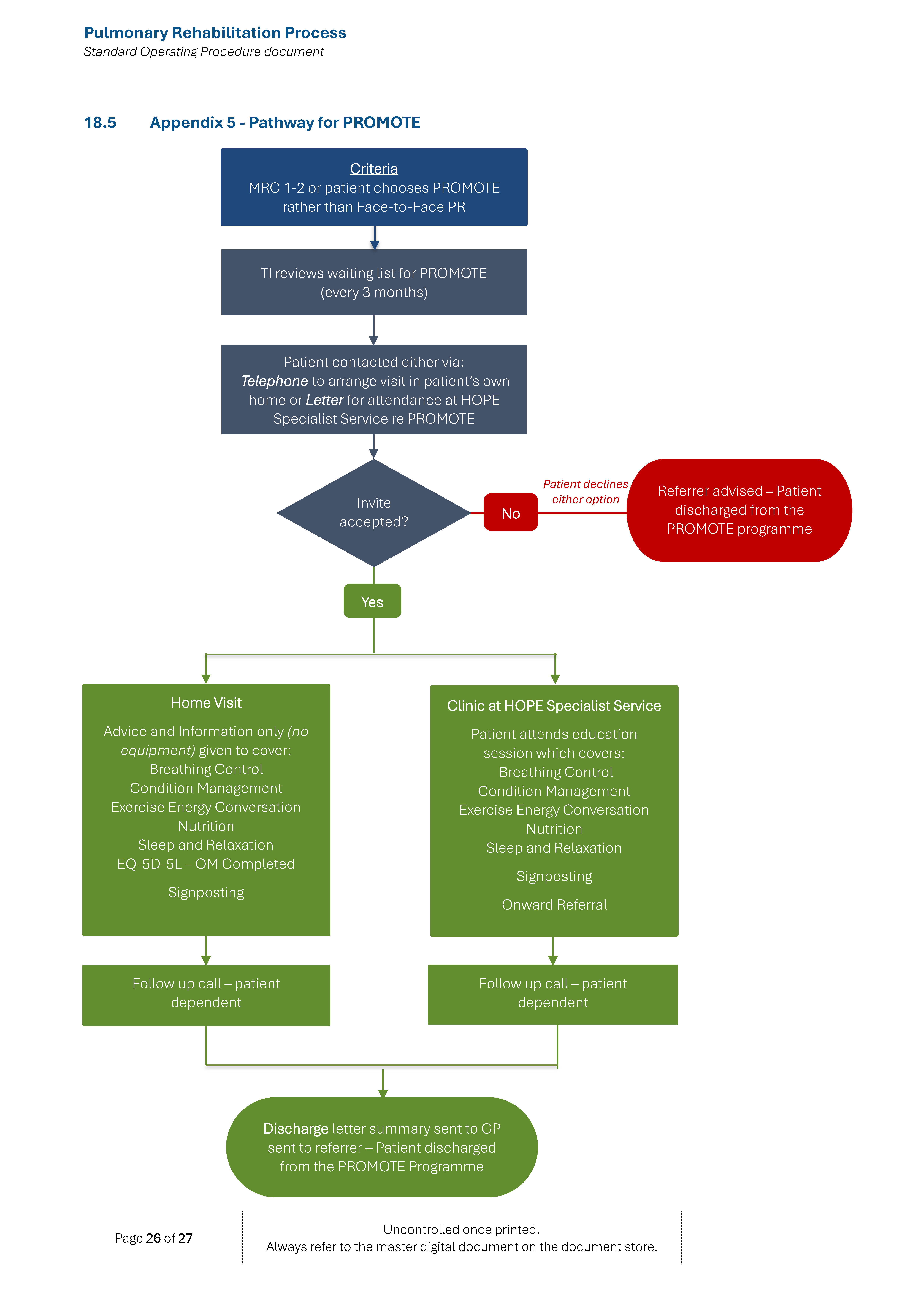
PROMOTE Process
PROMOTE is an educational and information session for newly diagnosed or highly functioning (MRC 1-2) patients with COPD or patients with a confirmed respiratory condition. The aim is to prevent disease and symptom progression and to ensure patients remain as active and independent as possible in managing their lung condition.
- MRC 1/2 or patient chooses PROMOTE intervention
- Patient placed on PROMOTE caseload and designated T.I to review every 3 months and to contact to offer out-patient appoint either 1:1 or group format or home visit
- Initial appointment to discuss individual needs to identify education sessions/resources toolkit required. These include breathlessness and management, exercises energy conservation, sleep and relaxation (all the education topics covered during PR programme)
- Outcome measures EQ-5D-5L completed to establish patient self-rated health
- Onward signposting/ referrals identified – e.g.: thrive, Cente4, Continence team
- Equipment is NOT provided and if identified by TI an onward referral to community therapy is completed
- Follow-up call or visit if required to summarise intervention
- Discharge summary letter to GP and discharged from care
Please refer to Appendix 5 for pathways.
Referral Criteria/Information
Referral Process: Competent Clinician
Referral pathways are via three patient pathways, either electronically through SystmOne, referral forms sent to generic email address at cpg.hopespecialistservice@nhs.net or via post.
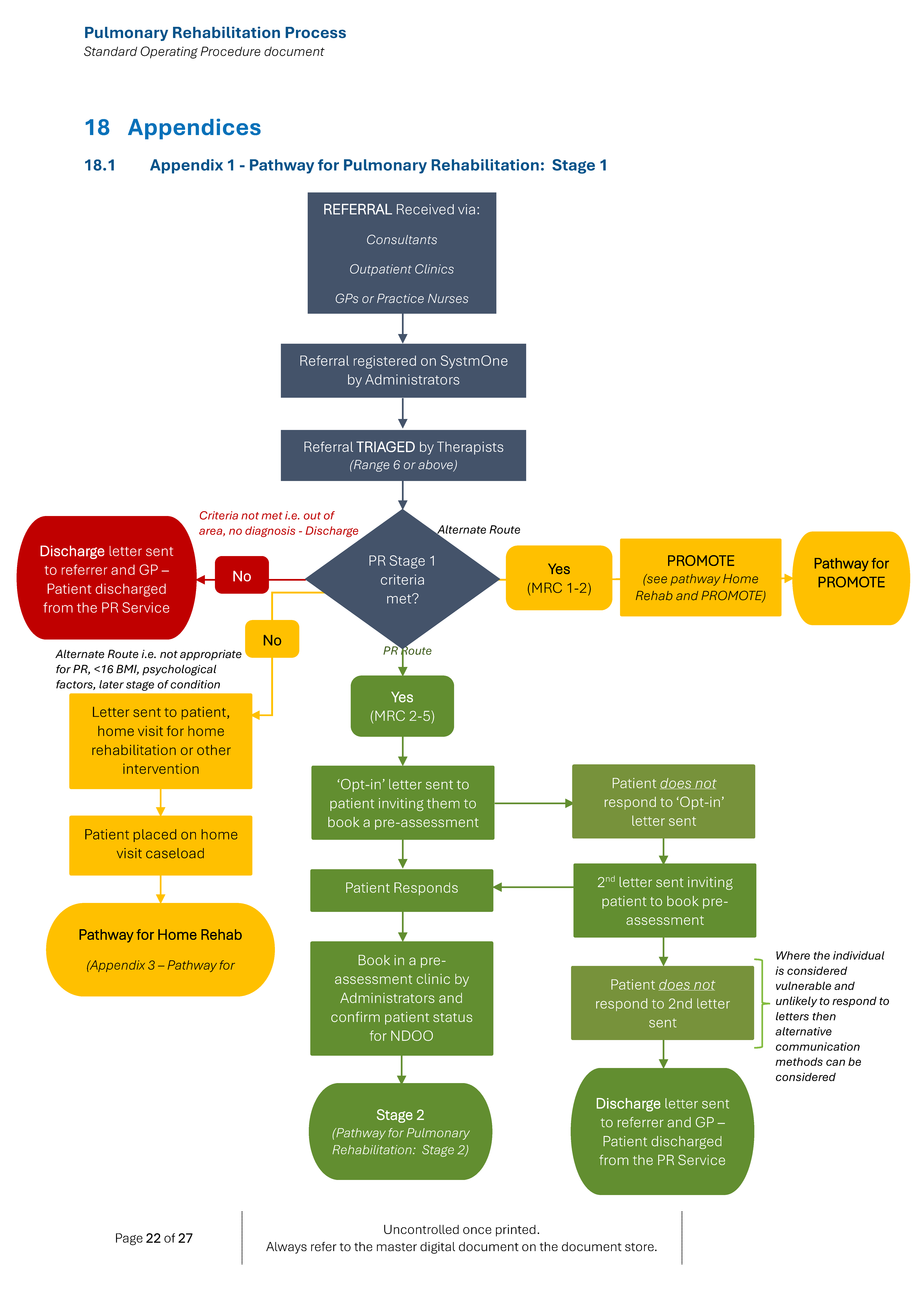
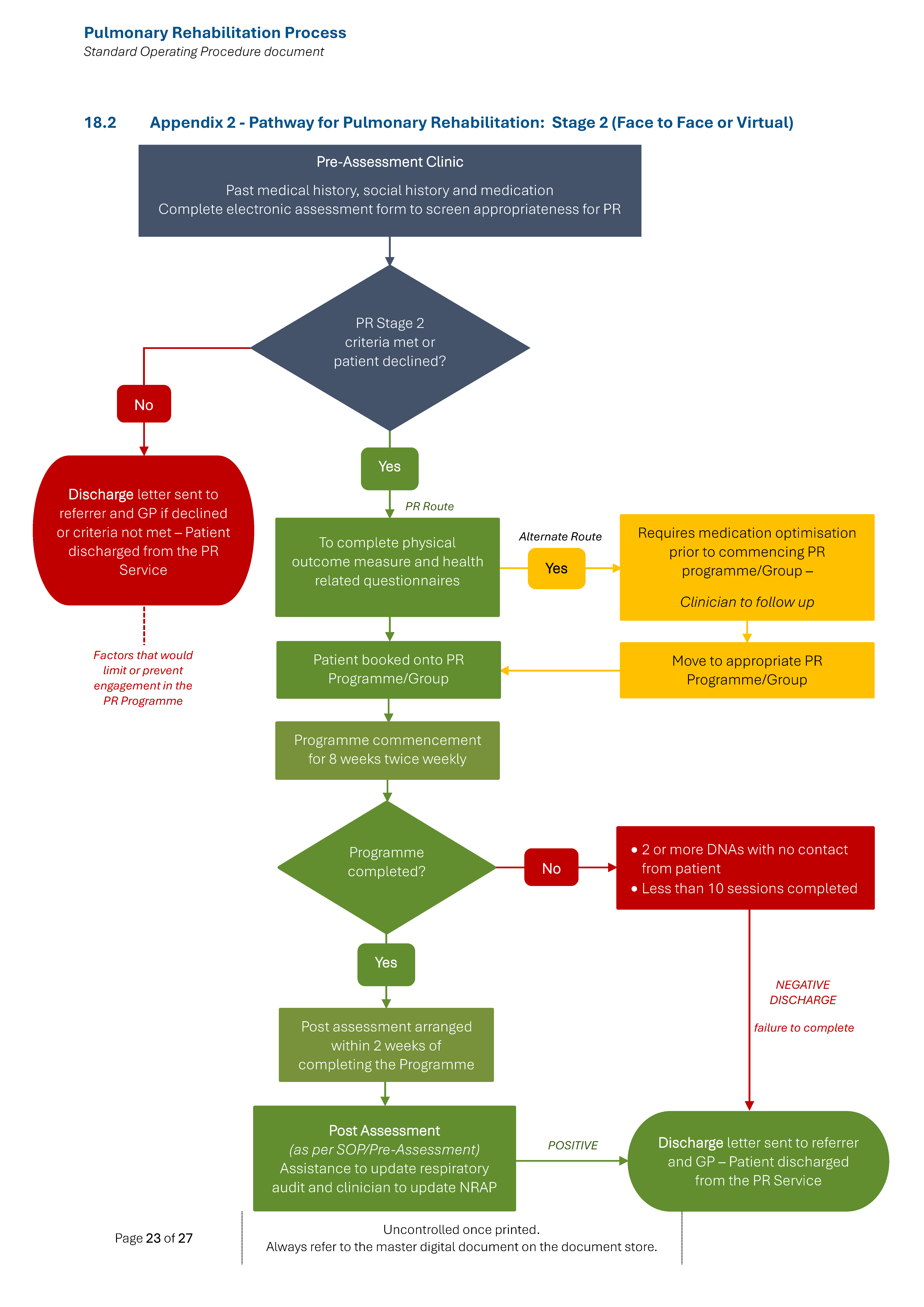
(a) Outpatient referral pathway: This refers to referrals for outpatients from all members of the primary and secondary care health care teams – refer to Appendices 1, 2 and 3.
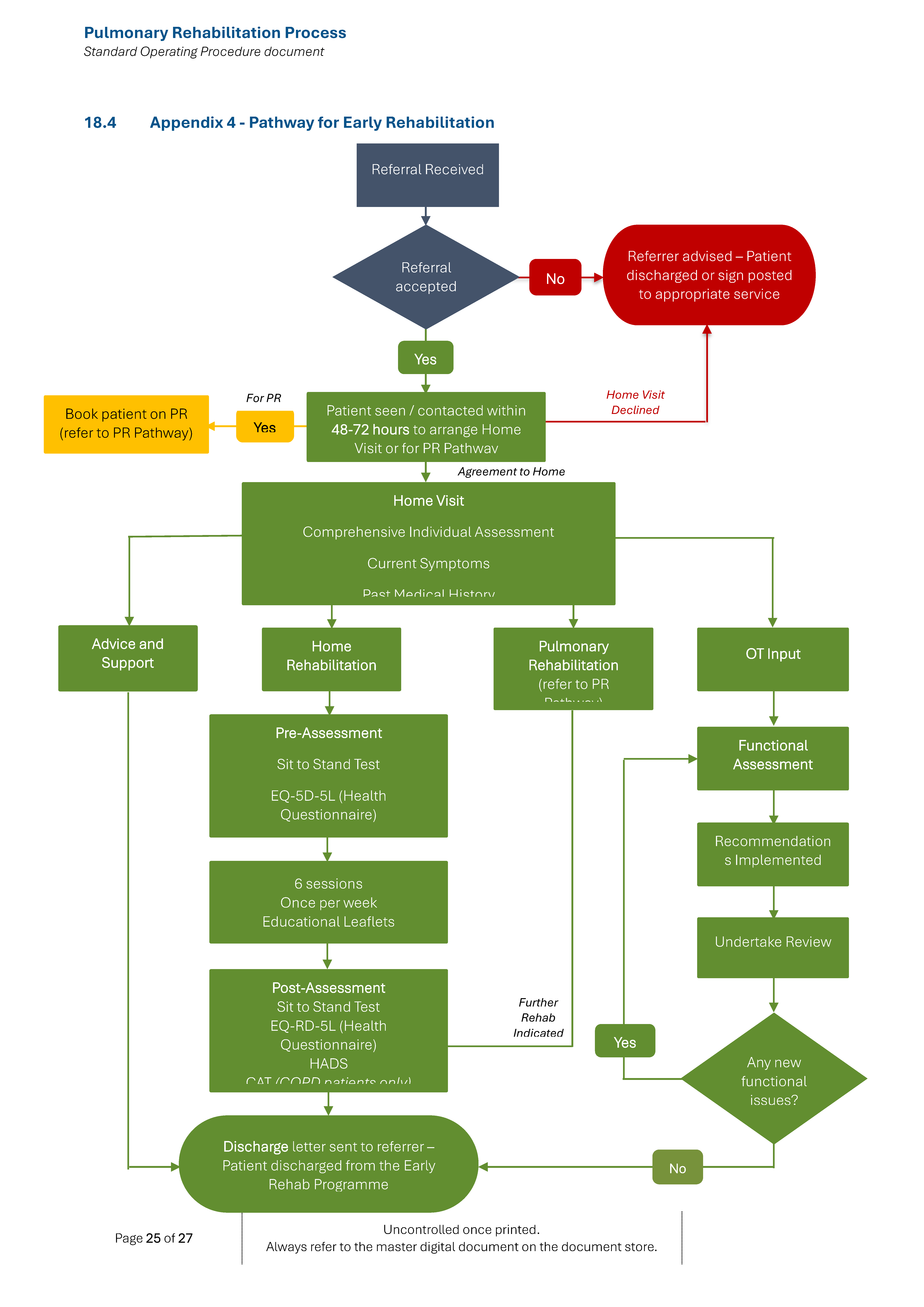
(b) Post exacerbation referral pathway: These are patients that have been recently admitted due to AECOPD and wish to undergo pulmonary rehabilitation following their discharge from hospital – refer to Appendix 4.
Assessment of Patients for Pulmonary Rehabilitation
All patients referred to the Pulmonary Rehabilitation Service will initially be offered a comprehensive one-to-one assessment by a member of the team of clinical specialists in Pulmonary Rehabilitation. This will include a review of the patient’s relevant medical and social history, an assessment of their current level of exercise performance and health status. Once this has been completed the patient is able to commence the pulmonary rehabilitation programme as appropriate.
Exercise Testing
Inclusion criteria:
- Any person without any contraindications absolute or relative to exercise testing as listed below in the Exclusion Criteria.
Exclusion Criteria:
Absolute Contraindications:
- A significant change in the resting ECG suggesting infarction or other acute cardiac events.
- Unstable angina
- Recent CVA <6/52
- Uncontrolled ventricular dysrhythmia that compromises cardiac function
- Third-degree A-V block
- Acute congestive heart failure
- Severe aortic stenosis
- HOCM
- Angina< 1 month post - PTCA/stent, post-CABG
- Known left main stem stenosis
- Suspected or known dissecting aneurysm
- Active or suspected myocarditis pericarditis
- Thrombophlebitis or intracardiac thrombi
- Recent systemic or pulmonary embolus
- Acute infection – Commenced Antibiotics and/or steroids in the last 1-2 days
Relative Contraindications:
- Left main coronary stenosis
- Resting diastolic blood pressure> 100 mm Hg or resting systolic blood pressure >180mm Hg.
- Moderate stenotic valvular heart disease
- Known electrolyte abnormalities (hypokalaemia, hypomagnesemia)
- Fixed rate pacemaker
- LBBB on ECG
- Angina < 1 month post – MI
- Frequent or complex ventricular ectopy
- Ventricular aneurysm
- Cardiomyopathy, including hypertrophic cardiomyopathy
- Uncontrolled metabolic disease (e.g. diabetes, thyrotoxicosis, or myxoedema)
- Chronic infectious disease (e.g. mononucleosis, hepatitis)
- Neuromuscular, musculoskeletal or rheumatoid disorders that are exacerbated by exercise
- Advanced or complicated pregnancy
(Adapted from American College of Sports Medicine – 2000)
- Increment Shuttle Walk Test
All patients meeting the inclusion criteria for the exercise component of PR will perform the Incremental (Singh et al, 1992) Shuttle Walking tests (refer to ISWT SOP) during the assessment. The outcome of these tests are used to calculate an individualised training prescription for each patient.
Assessment of Quadriceps Strength
Quadriceps strength of both legs is measured using a handheld dynamometer, unless contraindicated by osteoporosis, skin integrity or musculoskeletal reasons – refer to Quadriceps Muscle Strength Testing and Exercise Prescription SOP.
Assessment of Health Status
During the assessment, patients will complete a range of validated health status measures. These currently include:
(a) Chronic Respiratory Disease Questionnaire Self-Reported (Williams et al 2001 & 2003)
(b) Hospital Anxiety and Depression Scale (Zigmond and Snaith 1989)
(c) COPD assessment Test (CAT) (Jones et al 2009)
(d) EQ-5D-5L Source EuroQol Research Foundation. EQ-5D-5L User Guide, 2019. Latest version available from: https://euroqol.org/publications/user-guides
(e) General Anxiety Disorder – GAD 7 (Spitzer et al 2006)
(f) Patient Health Questionnaire PHQ 9(Spitzer et al 1999)
(g) Short Physical Performance Battery (SPPB) (Guralnik et al 1994)
8. Pulmonary Rehabilitation Programme
Programme
Programme Organisation
The Pulmonary Rehabilitation programme runs as a cohort programme every 8 weeks, twice weekly and rolling programme. Each session lasts for 2 hours with on average one and a half hours for exercise training and 30 minutes for the education programme. The cohort group runs for 16 sessions over 8 weeks, based at Val Waterhouse Centre and the ‘rolling’ programme, patients attend for 12 sessions, twice a week for six weeks. Patients then attend for a one-to-one discharge assessment and are given a written discharge plan, within a 2 week time frame following completion of PR.
Exercise Testing
Patients receive both aerobic and resistance training, twice weekly. Exercise training is individually prescribed and progressed from physical performance, health related questionnaires and patient goals obtained at baseline problems. Continuous and interval aerobic training are prescribed.
Walking training intensity is individually prescribed at a speed equal to 85% of the predicted VO2 peak calculated from the Incremental Shuttle Walking Test completed in the initial assessment. A target intensity of 60% of peak work rate is regarded as a minimum for endurance intensity. The aim is to accumulate 30-60 minutes per session aiming for 20-30 min of continuous activity. Patients are provided with a home exercise diary so they can record their progress. Patients’ progress is reviewed throughout with individual goals set in mid-session.
Patients are encouraged to complete an individualised home diary every day and one unsupervised home strength training session per week.
Procedure for Pre-Assessment Clinic Screening
Role of the Therapist (B6/7 Physiotherapist/Occupational Therapist)
- Check SystmOne to ensure compliance to patients National Data Opt Out (NDOO).
- Patients NDOO to NOT complete NRAP data.
- Discuss overview of the service and principles/commitment to PR programme.
- Consent to Ax following overview of clinic assessment, include explanation of consent to sharing.
- Document CPG consent section.
- Pressure leaflet discussed and issued.
- Complete respiratory assessment electronically on SystmOne or paper format (as a last resort and later scan to SystmOne) to include blood pressure, pulse rate, pulse oximetry, height, weight and BMI.
- If BMI <16 not appropriate for standard pulmonary rehabilitation. To offer alternative interventions (E.G. home visit for patient management plan/PROMOTE).
- BMI 16-18 offer and advise dietetic referral and monitor weight weekly.
- At halfway (week 4) if weight reduces (either unintentional or intentional weight loss) PR may be postponed until weight stable. If weight drops below BMI 16 to stop PR immediate effect and potentially discharge. Onward referral with consent.
- If BMI <16 or >30 offer referral on to Dietetics.
- If pulse oximetry indicates Sp02 <92% at rest (in accordance with NLaG oxygen (O2) Protocol and Referral Form) to consult with respiratory nurse specialists at DPoW. To provide patient with oxygen information.
- If patient demonstrates high levels of anxiety +/or depression >11 to continue to complete GAD7 (anxiety) PHQ9 (depression), if appropriate to do so or has had hospital admission due to COPD within last year consider referral to Open Minds for cognitive behavioural therapy, if appropriate.
- If further intervention is required that cannot be provided by the Hope Specialist Service, or the patient is inappropriate for pulmonary rehabilitation, refer back to the GP/referrer with rationale and appropriate recommendations. Update the patient and SystmOne notes for discharge summary.
- Physical Assessment to be completed including Cx Spine, Upper Limb and Lower Limb ROM and Strength. Lx Spine ROM, neuro screen, balance if indicated. Further MSK Assessments if required, will be undertaken during the course.
- To complete ‘Special’ questions and ‘Red Flag’ questions.
- Special questions around hyperventilation/Nijmegen questionnaire if indicated.
- To plan and undertake Balance assessment, if indicated as falls risk.
- Assessment of physical capabilities for exercise, to ensure individually tailored targets.
- Auscultation of the chest (physiotherapist)
- Refer to other disciplines as required (internally/externally).
- To follow up any ongoing or previous health issues that may affect ability/safety to exercise with appropriate staff e.g., controlled epileptic fits, cardiac history etc.
- Patients have to medically optimised prior to attending PR.
- If not appropriate for pulmonary rehabilitation, consider alternate interventions, better breather, PROMOTE and home rehab, if not absolutely contraindicated. Clearly documenting rationale for exclusion.
- If patient MRC 5b then discuss home rehab/better breather and perform SPPB/STS as outcome measures - consider discussion on advance care plan, to determine if previous discussion had.
- Clinician to complete body map/targets to include problem list, considerations, evidence base individual exercise programme - on T:/drive. To be attached to SystmOne post group.
- To add patient to list folder for NRAP
- To ensure patient is safe and has no contraindications for ISWT.
- Clinician to complete handover sheet for PR team prior to group commencing on T:/drive. To include PMH, considerations,1:1, walking speed, OT/PT specific input.
Blood Sugar Monitoring
- Diabetes must be stable.
- Ensure patients have eaten prior to exercise
- Patients monitor own blood sugars and blood testing kits, if appropriate.
- Patients to have emergency sweets etc, if at risk of hypoglycaemia.
- Patients must inform staff/lead clinician if experienced any hypoglycaemia in last 24 hours.
Role of Band 4 Technical Instructor assisting in Clinic and paperwork to be completed:
- Discuss and complete Disclaimer electronically.
- Describe the Incremental Shuttle Walk Test (ISWT) and follow SOP/protocol.
- To include practice run for ISWT, unless clinically inappropriate and to document on SystmOne and Audit spreadsheet
- Clinicians’ decision to determine who leads ISWT.
- To complete all pre-test information or supervise Volunteers documentation.
- Scores from the questionnaires should be checked and calculated correctly and then all relevant information copied across onto the summary box which is on the patient’s body map on the T:/drive.
- TI/Experienced Rehab Assistant is responsible for checking and signing off all documentation, including ‘buddies’ questionnaires.
- TI/Rehab Assistant to highlight HADS to clinician if 11 or above, and input in the OT section on the T:/drive.
- Admin team to update PR Audit excel sheet.
Outcome Measure Procedure
- Measure course – 2 cones to be 9-metres apart from back-to-back (marks in corridor).
- Ensure a chair is positioned at both ends of the course and explain to the patient to sit down when needed (or chair can be brought to patient).
- Ensure all sections of pre-assessment chart are completed.
- To complete objective muscle testing of quadriceps bi-laterally, 3 attempts with 10 seconds recovery in between each attempt– if deemed safe and appropriate by clinician. Highlight best of 3. Follow the Quadriceps Muscle Strength Testing and Exercise Prescription SOP.
- Patients should not undertake ISWT with acute chest infections requiring antibiotics and/or steroids in last 1-2 days. Clinician decision post 2 days of medication.
- Commence practise ISWT – discuss the standardised procedure with the patient and pay recording.
- Lengths to be recorded by buddy/staff and recovery time recorded, including sats, HR and BORG at each level.
- At least 5-minutes rest and complete ‘Sit to Stands’ in 1-minute - following protocol/SOP.
- Complete BP post ISWT/STS test.
- Complete Chronic respiratory questionnaire (CRQ’s)/COPD Assessment Tests (CAT)/Hospital Anxiety and Depression Score (HADS). Standard instructions used (CAT only for COPD patients).
- HADS score if 11 or more on anxiety to complete GAD7, Depression 11 or more to complete PHQ9. Use of clinical reasoning with these tools, as patients may currently take anti-depressants or be under Open Minds/Navigo Mental Health Services etc. Clinician decision.
- Maximum 30-minutes rest prior to undertaking the second ISWT, unless clinically inappropriate and document reasons.
- BP retaken prior to second ISWT. Complete ISWT as standardised instructors above/via SOP. Best result taken of the ISWT.
- BP retaken when breathing back to normal.
- Patient agrees to realistic, SMART goals.
- Patient asked if they feel ok to leave.
- Offer the patient a place on the course and ensure a course appointment letter (with dates/times etc.) is given or is sent via the postal service prior to the course commencing.
- Qualified therapist to complete Problem Chart, 1st target sheet and staff handover sheet.
Procedure if unable to complete one length of ISWT
- If the patient is unable to complete one length of IWST, undertake second ISWT to establish if one length can be achieved following learned effect. If unable to revert to SPPB Protocol and consider performing this if the patient is low level. Could consider Home Rehab/ and better breather as more appropriate options. Refer to Appendix 3 and 4 Pathways.
Additional Resources & Reference
Information sourced from: Pulmonary Rehabilitation Process SOP
- See above link for further information on:
- Pulmonary Rehabilitation Patient Structure
- Follow-up who DNA a Clinic/Pulmonary Rehabilitation Session
- Rehabilitation Plus
- Safety
- Managing Pulmonary Excercise Groups During Extreme Weather
Associated Documents
CPG SOP – Quadriceps Muscle Strength Testing and Exercise Prescription
CPG SOP – Pulmonary Rehabilitation: 1 Minute Sit to Stand Test
CPG SOP – Incremental Shuttle Walk Test (ISWT)
CPG SOP – Rehabilitation Plus
References
Bolton C, Bevan-Smith E, Blakey J, Crave P, Elkin S, Garrod R et al. BTS guidelines on Pulmonary Rehabilitation in Adults. Thorax.(2013)68:ii1–ii30.
British Thoracic Society Reports . BTS Quality Standards for Pulmonary Rehabilitation in Adults (2014) Vol. 6, No.2
American College of Sports Medicine. "Guidelines for Exercise Testing and Training of the American College of Sports Medicine." (2000): 85-88.
Singh, S, Morgan, M, Scott, S, Walters, D, Hardman, A. Development of a shuttle walking test of disability in patients with chronic airways obstruction. Thorax (1992) 47;12 : 1019-24.
Revill, S, Morgan, M, Singh, S, Williams, J, Hardman, A. The endurance shuttle walk: a new field test for the assessment of endurance capacity in chronic obstructive pulmonary disease. Thorax (1999) 54;3 : 213-22.
Williams, J, Singh, S, Sewell, L, Guyatt, G, Morgan, M. Development of a self-reported Chronic Respiratory Questionnaire (CRQ-SR). Thorax (2001) 56;12 : 954-59.
Jones, P, Harding, G, Berry, P, Wiklund, I, Chen, W-H, Kline Leidy, N. Development and first validation of the COPD Assessment Test Eur Respir J (2009) 34:648-654.
Vincent E, Sewell, L., Wagg K, Deacon S, Williams, J., and Singh, S. J. Measuring a change in self-efficacy following Pulmonary Rehabilitation: An evaluation of the PRAISE tool. Chest (2011) 140;6 1534-1539.
Zigmond, A. S. and R. P. Snaith. The hospital anxiety and depression scale. Acta Psychiatr.Scand. (1983) 67;6 : 361-70.
White, R, Walker, P, Roberts, S, Kalisky, S, White, P. Bristol COPD Knowledge Questionnaire (BCKQ): testing what we teach patients about COPD. Chron.Respir.Dis. (2006) 3;3 : 123-31.
Associated Policies
Specialties
Places covered by
- North East Lincolnshire
Hospital Trusts