HNY Policy and Pathway Repository - York
Erectile dysfunction (impotence)
Definition/Description
Erectile dysfunction is defined as the persistent inability to attain and maintain an erection sufficient to permit satisfactory sexual performancei . Erectile dysfunction is a symptom and not a disease, therefore it is important to identify any underlying disease or condition that could be causing it. See below for details on causes of ED.
Facts
- Significant impact on quality of life and effects up to 52% of men (40-70yrs)
- Steep age-related increase.
- Complete impotence from 5% of 40yr olds to 15% of 70yr olds.
- Only 10-20% solely psychogenic
Red Flag Symptoms
None provided
Guidelines on Management
History Taking
The main goal here is to ascertain the underlying cause (see diagrams 1-3)
- Relationship status (current and past) and sexual orientation.
- Present and previous erection quality (including erections during sex, morning erections and masturbatory erections)
- Any ejaculatory and orgasm dysfunction.
- Issues with sexual aversion or pain, or issues for his partner (including menopause or vaginal pain).
- Use of alcohol, tobacco, and illicit drugs (including cannabis), and treatments already tried.
- Activity levels
- Energy levels, loss of libido, loss of body hair, or spontaneous hot flushes (symptoms of hypogonadism).
Examination
- CVS assessment including body weight, waist circumference, heart rate, and BP.
- Examination of the genitalia if appropriate? hypogonadism? Peyronie's disease?
- Also check for gynaecomastia and reduced body hair.
- A DRE is recommended if there are symptoms of an enlarged prostate. Rarely, the enlarged prostate obstructs the flow of ejaculate causing prolonged and intermittent ejaculation.
Investigations
- Check the Q-RISK
- Urine Dipstick
- For Peyronie's disease: consider referring to andrology services for further management; penile rehabilitation/ surgery (please advise the patient to attend with photo of erected penis for assessment)
- Bloods to request: HBA1c, Lipid profile and total testosterone
- If the total testosterone level is low then repeat sample sent to lab including: FSH, LH, Prolactin, Testosterone (9am) and SHBG
- If the repeat bloods are abnormal, then consider referral to andrology services for primary hypogonadism and endocrinology if secondary hypogonadism or suspicion of pituitary gland abnormalities. Please note that if patient being considered for testosterone therapy, then the following additional tests are required at baseline: PSA, LFTs and FBC
Management:
Self Care
NICE state: Counsel the man that erectile dysfunction usually responds well to a combination of lifestyle changes and drug treatment. Advise, where applicable, that he should:
- lose weight (important as obesity strongly associated with ED, P< 0.006)
- stop smoking 40% of smokers have ED, compared to 28% in general population
- reduce alcohol consumption and
- increase exercise. (lack of exercise strongly associated with ED (P<0.01)
Men who initiated physical exercise and weight loss have up to 70% improvement (note: cycling more than 3 hours per week may cause dysfunction though well fitted saddles that specifically protect the pudendal nerve may help)
Advise the man not to take unlicensed herbal remedies for erectile dysfunction as they may contain prescription-only medicines which may be contraindicated or interact with prescribed medication.
Advice and support is also available from the Sexual Dysfunction Association
Diagnose and treat underlying cause (see diagrams 1-3)
Treatment of Erectile Dysfunction in Primary Care:
1. Give the self-care advice as detailed above.
2. Generic sildenafil can be prescribed to any NHS patient without the ‘SLS’ restrictions:
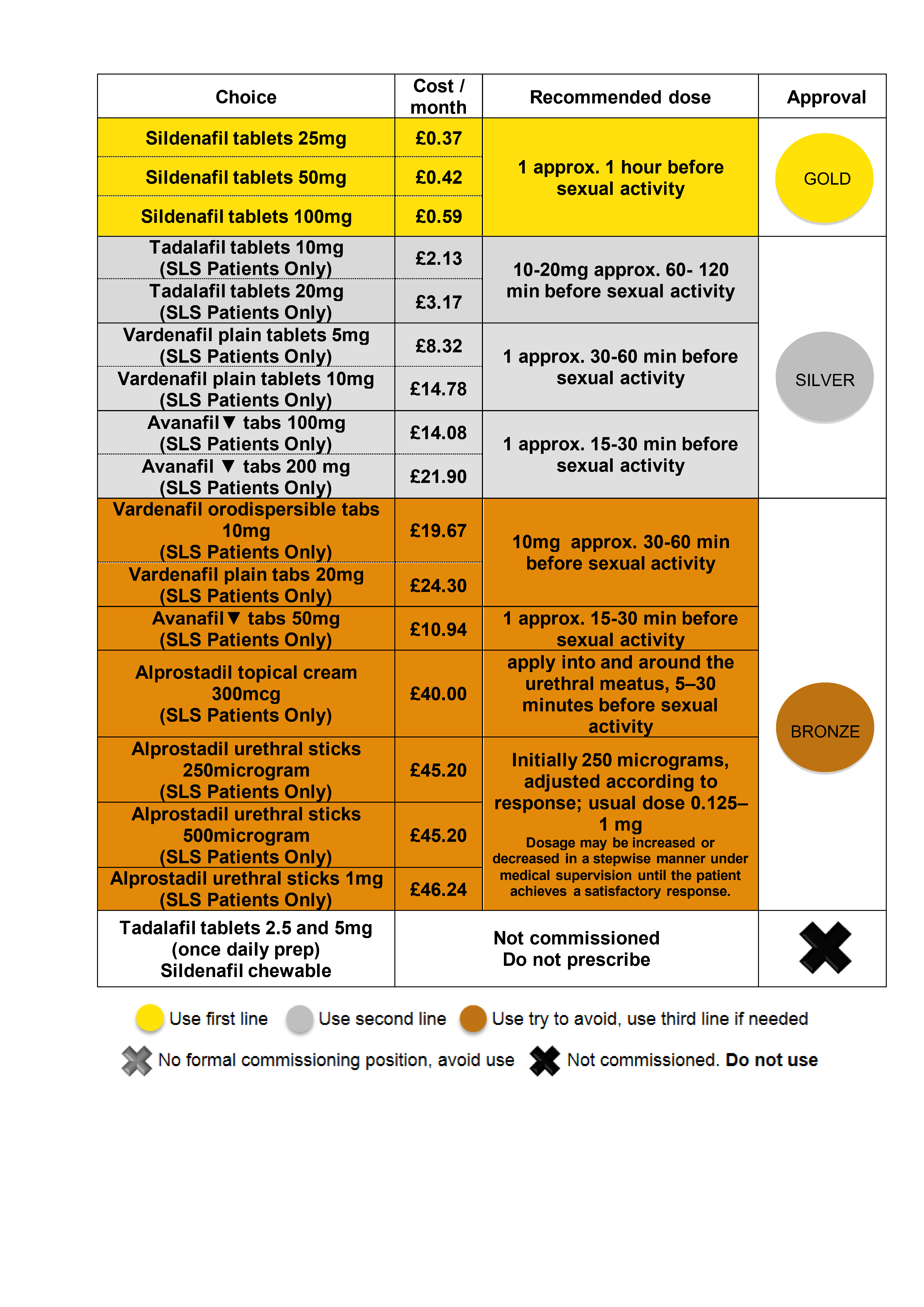
- Prescribe PRN oral phosphodiesterase-5 (PDE-5) inhibitors according to the CCG’s medal ranking table below.
- Ensure the man is aware that PDE-5 inhibitors are not initiators of erection but require sexual stimulation in order to facilitate erection.
- Warn patients to seek advice if he has an erection lasting more than four hours (priapism). NICE say to admit if so. NHS advice on self help is here where it says go to A&E if the erection lasts more than 2 hours.
- NICE states patients should receive eight doses (over 8 weeks of a PDE-5 inhibitor) at a maximum dose with sexual stimulation before being classified as a nonresponder.
- Only if these are contra-indicated, (e.g. concurrent prescribing of nitrates, recent CVA or MI or unstable angina, or if a full trial of all the oral phosphodiesterase-5 (PDE-5) inhibitors results in an inadequate response) try topical alprostadil cream. This currently costs £10 per single use prescription. There is further information from NICE here - Evidence Summary of New Medicines. Alprostadil urethral sticks may also be tried thereafter, a medical professional should instruct each patient on the correct use of this medicine.
3. The following are not prescribable on the NHS: Viagra® (brand only), tadalafil (Cialis®), vardenafil (Levitra®), avanafil (Spedra®) and Alprostadil (Caverject®, Viridal®Duo, Vitaros®, MUSE®) unless they are for men defined in selected list scheme (SLS) criteria who:
- Have diabetes, multiple sclerosis, Parkinson's disease, poliomyelitis, prostate cancer, severe pelvic injury, single-gene neurological disease (for example Huntington's disease), spina bifida, or spinal cord injury or,
- Are receiving renal dialysis for renal failure or,
- Have had radical pelvic surgery, prostatectomy (including transurethral resection of the prostrate), or a kidney transplant or,
- Were receiving Caverject®, Erecnos®, MUSE®, Uprima®, Viagra®, Cialis®, or Viridal® at the expense of the NHS on 14 September 1998.
The prescriber must endorse the prescription with the reference "SLS". (Drug Tariff November 2018)
4. Up to ONE treatment a week for any of the treatments is all that should be supplied on the NHS locally. Additional supplies can be made on private prescription.
5. For patients that do not fulfil the ‘SLS’ conditions above and do not tolerate generic sildenafil, these patients may request a private prescription from their GP. The GP can prescribe a private prescription for any of the medication listed in the medal ranking table, if they feel this is clinically appropriate.
Viagra Connect® (sildenafil) is another treatment option that can be purchased from pharmacies and is available without a prescription. This may be a suitable option for patients taking sildenafil prescribed on the NHS and would like further supplies. This costs around £19.99 for 4 tablets.
(See image A below)
Other Prescribing Information:
Substitute where possible medication that may contribute to erectile dysfunction where a temporal link can be established.
NICE state whilst there is a lack of head to head RCTs sildenafil, tadalafil and vardenafil are probably equally effective so prescribers are recommended to follow GMC advice to make good use of the resources available to you and prescribe using the medal ranking table below.
About 75% of men using PDE-5 inhibitors will have improved erections. The drugs have an NNT of 2 - approximately two men need to be treated for one man to benefit.
Assess whether a patient is eligible for an NHS prescription. See guidance here. Generic sildenafil is now (since August 2014) no longer in the ‘SLS’ list meaning that restrictions on its use are lifted and can be prescribed by GPs on FP10 for any indication for ED, including severe distress.
Prescribe the lower dose of the drug initially, and consider titrating upwards if this is ineffective (see NICE guidance on further Follow up).
NICE state: ‘a man with erectile dysfunction should receive eight doses of a PDE-5 inhibitor at a maximum dose with sexual stimulation before being classified as a non-responder’
Other adverse effects are:
Adverse effect |
Sildenafil (n = 5918) |
Tadalafil (n = 804) |
Vardenafil (n = 2203) |
Headache |
14.6 |
14 |
14.5 |
Flushing |
14.1 |
4 |
11.1 |
Dyspepsia |
6.2 |
10 |
3.7 |
Rhinitis |
2.6 |
5 |
9.2 |
Back pain |
0.0 |
6 |
0.0 |
Visual disturbance |
5.2 |
0 |
0.0 |
Use in Coronary Heart Disease
The British Society of Sexual Medicine states an ED patient with no cardiac symptoms; is a cardiac patient, unless this has been excluded. NICE advises that most men with CHD can safely resume sexual activity and use phosphodiesterase-5 (PDE-5) inhibitors. The exceptions are men with:
- Unstable heart disease.
- A history of recent myocardial infarction.
- Poorly compensated heart failure.
- Unstable dysrhythmia
Causes:
Erectile dysfunction is a symptom and not a disease, therefore it is important to identify any underlying disease or condition that could be causing it There are physical, psychological and hormonal causes.
Physical causes of EDii
Vasculogenic
|
Neurogenic
|
Anatomical / Structural
|
Hormonal
|
Psychological causes of EDiii
Predisposing
- Lack of Sexual Knowledge
- Past Sexual Problems
- Relationship Problems
- Religious / Cultural Beliefs
- Restrictive Upbringing
- Unclear Gender / Sexual Preference
- Sexual Abuse
- Physical / Mental Ill-health
Precipitating
- New Relationship
- Acute Relationship Problems
- Family / Social Pressures
- Pregnancy / Childbirth
- Significant Life Events
- Acute physical / mental illness
- Lack of knowledge about normal
- ageing / body changes
Maintaining
- Relationship Problems
- Poor Communication between partners
- Chronic physical / mental health problems
Drug causes of EDiv
Diuretics – thiazides, spironolactone
Anti-hypertensives – methyldopa, clonidine, beta blockers, verapamil
Anti-depressants – SSRIs, Lithium, TCAs, MAOIs
Anti-psychotics – chlorpromazine, haloperidol
H2 antagonists – cimetidine, ranitidine
Cytotoxics – cyclophosphamide, methotrexate
Anti-arrhythmics – disopyramide
Anti-convulsants – carbamazepine
Hormones – prednisolone, cyproterone, 5-alpha reductase inhibitors, e.g. finasteride
Referral Criteria/Information
If there is an inadequate response after all medical treatments refer to Urology
ED Clinic (through Choose & Book) please include in referral:
- Life style advice given and changes made
- Duration, PMH (DM , HT , IHD / on GTN),
- Genital examination and PR (if appropriate)
- Tests: HbA1c, lipid profile, total testosterone
- PDE-5 therapies (list all tried) 8 tablets including max does + alprostadil cream: Failed / contraindication
Information on Vacuum Pumps, if recommended by specialists
They cost around £100-£200 depending on the model The drug tariff (November 2018) states: They can only be prescribed "on the NHS" if the patient has diabetes, multiple sclerosis, Parkinson's disease, poliomyelitis, prostate cancer, severe pelvic injury, single gene neurological disease, spina bifida, spinal cord injury; or a man who is receiving treatment for renal failure by dialysis; or a man who has had the following surgery prostatectomy, radical pelvic surgery, renal failure treated by transplant.
The prescriber endorses the face of the prescription form with the reference "SLS".
If none of the above apply they should be prescribed privately.
Additional Resources & Reference
References
i. British Society for Sexual Medicine, 2009; Wespes et al, 2012
ii. British Society for Sexual Medicine, 2009; Wespes et al, 2012
iii. Adapted from Hackett et al, 2008]
iv. Hackett et al, 2008; British Society for Sexual Medicine, 2009; Wespes et al, 2012
v. NICE CKS Dec 2017 https://cks.nice.org.uk/erectile-dysfunction#!prescribinginfosub
Associated Policies
Specialties
Places covered by
- vale-of-york
Hospital Trusts
- york-and-scarborough-teaching-hospitals